

FOR IMMEDIATE RELEASE – September 28, 2018 – Washington, D.C. – The American Childhood Cancer Organization (ACCO), the soleU.S. member of Childhood Cancer International (CCI) provided its overwhelming support today for the World Health Organization’s (WHO)  announcement of its new global initiative to address the disparity between childhood cancer survival in low-middle versus high-income countries. The announcement came at the United Nations (UN) General Assembly’s side-meeting on childhood cancer which was organized by the Missions of the Republic of Uzbekistan, the Hashemite Kingdom of Jordan, El Salvador, the Republic of Moldova, the Kingdom of Morocco, the Republic of Philippines and the Russian Federation.
announcement of its new global initiative to address the disparity between childhood cancer survival in low-middle versus high-income countries. The announcement came at the United Nations (UN) General Assembly’s side-meeting on childhood cancer which was organized by the Missions of the Republic of Uzbekistan, the Hashemite Kingdom of Jordan, El Salvador, the Republic of Moldova, the Kingdom of Morocco, the Republic of Philippines and the Russian Federation.
Funded through a generous donation from St. Jude Children’s Research Hospital, the WHO Global Initiative for Childhood Cancer partners with national and international *stakeholders including CCI to provide leadership and technical assistance to support governments in building and sustaining high-quality childhood cancer programs.
Each year, more than 300,000 children ages birth to 19 years are diagnosed with cancer around the world. Approximately 8 in 10 of these children live in low and middle-income countries where their survival rate is often near 20%. This is in stark contrast to high-income countries, where cure rates exceed 80% for many common childhood cancers.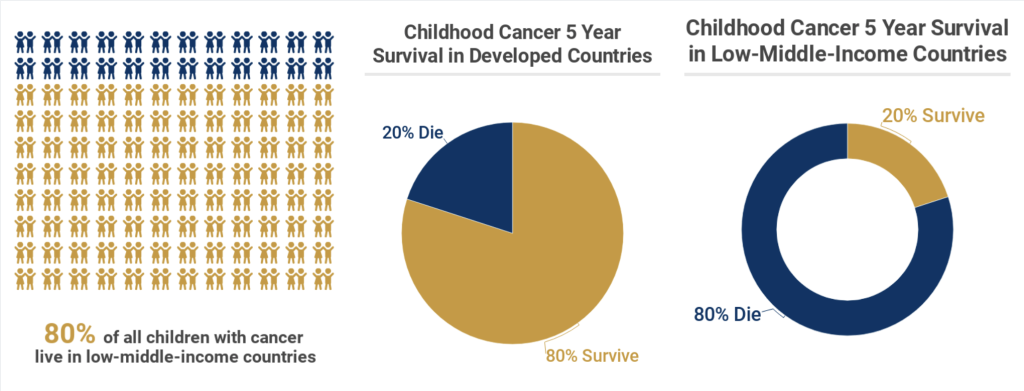
How urgent is this global initiative? “Childhood cancer is the number one non-communicable disease (NCD) cause of death in children globally,” said Ruth Hoffman, ACCO’s Chief Executive Officer, and President of Childhood Cancer International. “Childhood cancer has no borders. Why should childhood cancer treatments and cures? Even in the U.S. the majority of children with cancer continue to be treated with old drugs that were developed in the 1950’s, ‘60’s and 70’s. These drugs cost very little yet are too often unavailable to the majority of children with cancer in the world who happen to live in low to middle income countries. With increased access to essential childhood cancer medicines and radiation, children can be cured of their disease regardless of where they live in the world.” Ms. Hoffman will continue to represent the voice of the families of children with cancer as a member of the WHO Global Initiative for Childhood Cancer.
- Increase political commitment and capacity of countries to deliver best practices in childhood cancer diagnosis and treatment;
- Support governments to develop high-quality cancer centers as well as develop standards and tools to guide the planning and implementation of interventions for early diagnosis, treatment and palliative and survivorship
care inclusive of the needs of childhood cancers; - Improve access to affordable essential child cancer medicines and technologies;
- Support governments to safeguard families of children with cancer from social isolation and financial ruin as a result of cancer care;
- Prioritize cancer as a child health priority and increase available funding at the national and global levels.
This initiative is founded on the World Health Assembly’s resolution Cancer Prevention and Control through an Integrated Approach (WHA70.12), which urges governments and WHO to accelerate action to achieve the targets specified in the Global Action Plan and 2030 UN Agenda for Sustainable Development to reduce premature mortality from cancer.
Actions to increase childhood cancer survival today represent effective and tangible steps as part of the broader fight against non-communicable diseases – steps that will catalyze global efforts to transform childhood cancer outcomes worldwide and ultimately save many more lives of children, now and for years to come.
*Some Stakeholders include: The International Society of Pediatric Oncology (SIOP), Intenational society of pediatric oncologists, Union for International Cancer Control (UICC), International Atomic Energy Agency (IAEA), International Agency for Research on Cancer (IARC), Sick Kids Hospital of Toronto, Texas Children’s Hospital, World Bank, Pediatric Oncology Rally to Transform Access to Global Essentials (PORTAGE), Friends of Cancer Patients (FOCP), Chai Clinton Health Access Initiative (CCHAI), BIO Ventures for Global Health (BVGH), Pharmaceutical Industry, International Federation of Pharmaceutical Manufacturers & Associations (IFPMA)
_________________________________
The American Childhood Cancer Organization was founded in Washington, D.C. in 1970 by parents of children and adolescents diagnosed with cancer to advocate for their needs and support research so every child survives and leads a long and healthy life. The U.S. largest grassroots organization at the forefront of the crucial battle against childhood cancer, the ACCO is dedicated to shaping policy, supporting research, raising awareness and providing educational resources and innovative programs to children with cancer, survivors and their families. Since its inception, the ACCO has helped support more than half a million families affected by childhood cancer. ACCO now has 35 local ACCO affiliates known as Founding Hope chapters throughout the United States. www.acco.org.
Childhood Cancer International (CCI) was founded in 1994 and is recognized as the largest patient support organization for childhood cancer in the world. Comprised of 188 member organizations in 98 countries, CCI represents the voice of children and adolescents with cancer, childhood cancer survivors and their families globally. Operating as a non-State Actor in official relations with the World Health Organization (WHO), CCI engages with the WHO as well as international develo
pment organizations, policy-makers, civil society organizations, research and medical professionals to advocate for the rights of children and adolescents with cancer and prioritize childhood cancer as an integral part of the local, national and global child health and development agenda. www.childhoodcancerinternational.org
FOR MORE INFORMATION OR TO SET UP AN INTERVIEW: Contact Ruth Hoffman, Chief Executive Officer, American Childhood Cancer Organization and President, Childhood Cancer International. rhoffman@acco.org; 202-262-9949.
 Meet Beckham, one of our ambassadors for the month of September. He is a goofy 8 year old currently being treated for Stage 4 Neuroblastoma at Memorial Sloan Kettering in New York City. Beckham was diagnosed on September 11, 2013 at the age of 3. A few weeks prior to his diagnosis, Beckham was playing with his sister and they banged their heads together. This resulted in Beckham’s black eyes. His mom remembers looking at pictures from that time and seeing his eyes starting to darken.
Meet Beckham, one of our ambassadors for the month of September. He is a goofy 8 year old currently being treated for Stage 4 Neuroblastoma at Memorial Sloan Kettering in New York City. Beckham was diagnosed on September 11, 2013 at the age of 3. A few weeks prior to his diagnosis, Beckham was playing with his sister and they banged their heads together. This resulted in Beckham’s black eyes. His mom remembers looking at pictures from that time and seeing his eyes starting to darken.  At first, doctors didn’t think Beckham had cancer, they went through many diagnoses, everything from mono to anemia. The doctors were not convinced and decided to do a bone marrow biopsy which revealed that Beckham had tumors throughout his body and bone marrow.
At first, doctors didn’t think Beckham had cancer, they went through many diagnoses, everything from mono to anemia. The doctors were not convinced and decided to do a bone marrow biopsy which revealed that Beckham had tumors throughout his body and bone marrow.  Treatment was aggressive and as a result Beckham started chemotherapy. The doctors performed a resection of the main tumor and radiation to his skull in Utah which resulted in soft tissue tumors and bone marrow clearing well but the tumors in his bones had hardly changed. Beckham’s mom recalls going onto a Facebook group for Neuroblastoma and was urged to take him for a second opinion at Memorial Sloan Kettering. February 2014 was the first trip to NYC where Beckham received MIBG therapy, NK cell therapy, radiation, 3f8 antibioties, cryotherapy surgery, numerous rounds of chemotherapy and surgery to remove lymph nodes in his upper right underarm and chest.
Treatment was aggressive and as a result Beckham started chemotherapy. The doctors performed a resection of the main tumor and radiation to his skull in Utah which resulted in soft tissue tumors and bone marrow clearing well but the tumors in his bones had hardly changed. Beckham’s mom recalls going onto a Facebook group for Neuroblastoma and was urged to take him for a second opinion at Memorial Sloan Kettering. February 2014 was the first trip to NYC where Beckham received MIBG therapy, NK cell therapy, radiation, 3f8 antibioties, cryotherapy surgery, numerous rounds of chemotherapy and surgery to remove lymph nodes in his upper right underarm and chest.  Beckham has had two central lines and is on his third port. “He has endured four relapses, the most recent being March of 2018 and his doctors say he is a miracle boy.”
Beckham has had two central lines and is on his third port. “He has endured four relapses, the most recent being March of 2018 and his doctors say he is a miracle boy.” 


 Fortunately, Braeden is facing treatment like a little soldier; the only side effect he has experienced was hair loss, which he doesn’t seem to mind. Kendra notes that everytime he goes into the hospital, the nurses fight to work with him and that he charms them. She said when Brae is at home, he loves to watch tv with his big brother and play outside. He’s particularly interested in art and loves to paint. When he goes to the hospital you can usually find him in the art room playing with the popsicle sticks and paint.
Fortunately, Braeden is facing treatment like a little soldier; the only side effect he has experienced was hair loss, which he doesn’t seem to mind. Kendra notes that everytime he goes into the hospital, the nurses fight to work with him and that he charms them. She said when Brae is at home, he loves to watch tv with his big brother and play outside. He’s particularly interested in art and loves to paint. When he goes to the hospital you can usually find him in the art room playing with the popsicle sticks and paint.  There are nearly 5,000 new diagnoses of childhood leukemia every year in the United States, making this so-called “rare” disease the most common type of childhood cancer. In fact, childhood leukemia currently accounts for almost one-third of all childhood cancer diagnoses. Thanks to amazing advances in the efficacy of today’s treatment protocols, the majority of children diagnosed with leukemia today can expect to make a full recovery. The 5-year survival rates for the two main forms of leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—are greater than 85% and about 60-70% respectively.
There are nearly 5,000 new diagnoses of childhood leukemia every year in the United States, making this so-called “rare” disease the most common type of childhood cancer. In fact, childhood leukemia currently accounts for almost one-third of all childhood cancer diagnoses. Thanks to amazing advances in the efficacy of today’s treatment protocols, the majority of children diagnosed with leukemia today can expect to make a full recovery. The 5-year survival rates for the two main forms of leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—are greater than 85% and about 60-70% respectively.

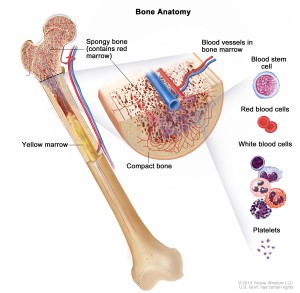 Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow.
Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow. Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL.
Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL. Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy.
Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy. Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally.
Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally. Any discussion of prognosis or outlook is usually based on five-year survival rates, or the percentage of children with a specific type of cancer who live at least five years after their initial diagnosis. These numbers are based on studies performed at least five years ago, and so may not reflect improvement in treatment options for some types of cancers. Moreover, these numbers are merely averages and do not indicate the outlook or prognosis for your specific child. Your child’s oncologist will be able to give you a better understanding of your child’s unique case based on his or her type of cancer, age, general health, and response to treatment.
Any discussion of prognosis or outlook is usually based on five-year survival rates, or the percentage of children with a specific type of cancer who live at least five years after their initial diagnosis. These numbers are based on studies performed at least five years ago, and so may not reflect improvement in treatment options for some types of cancers. Moreover, these numbers are merely averages and do not indicate the outlook or prognosis for your specific child. Your child’s oncologist will be able to give you a better understanding of your child’s unique case based on his or her type of cancer, age, general health, and response to treatment.