

Detection and Diagnosis
 The brain and the spinal cord make up what is known as the Central Nervous System (CNS) and together, they control nearly all of our body’s normal functions. The brain is composed of three major parts.
The brain and the spinal cord make up what is known as the Central Nervous System (CNS) and together, they control nearly all of our body’s normal functions. The brain is composed of three major parts.
- The cerebrum controls thinking, emotions, speech, learning, problem solving, and voluntary movement.
- The cerebellum controls movement, balance, and posture.
- The brain stem connects the brain to the spinal cord. It is responsible for autonomic functions such as breathing and heart rate, as well as the muscles and nerves that enable us to see, hear, walk, talk, and eat.
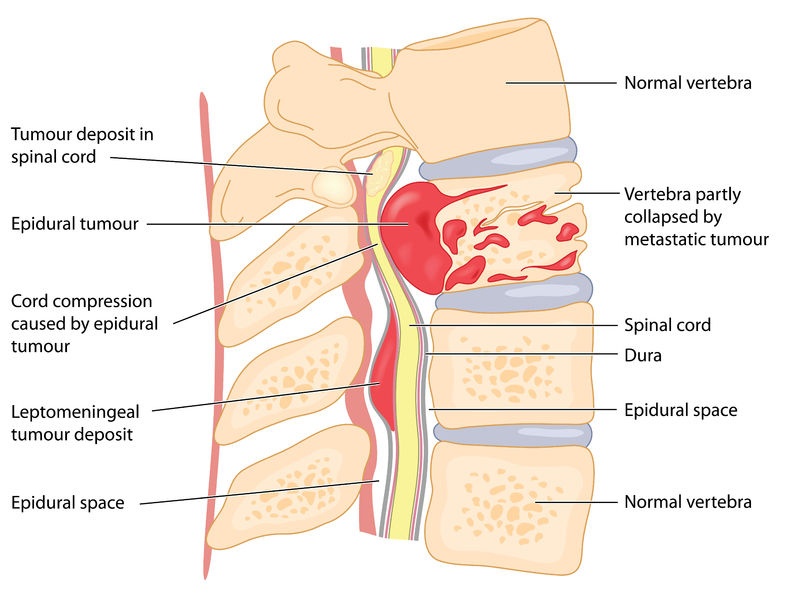
The spinal cord is the delicate column of nerve tissues contained within the “back bone”, the collection of vertebrae that protect the nerves. These nerves carry the critical messages between the brain and the body that enable the body to function normally and properly.
A spinal cord tumor is a growth of abnormal cells within the spinal cord. A tumor forms as cells grow and/or replicate too quickly, or do not die at the correct time. The tumor may be either malignant (cancerous) or benign (non-cancerous); however, this distinction is less critical when dealing with spinal cord tumors because both types of tumors can—as they grow—press on and constrict the healthy tissues of the spinal cord and impede their normal functioning. Thus, both benign and malignant tumors can cause similar types of symptoms. Usually, detection and diagnosis of a spinal cord tumor occurs only after a child begins to show unusual symptoms indicating a potential health concern.
The symptoms of a spinal cord tumor may vary widely from child to child, depending on individual circumstances such as exactly where the tumor is growing, how it is pressing on other nerves and tissues, how quickly it is growing, and the age and development of the child. Some of the more common signs of a spinal cord tumor may be issues such as:
- Pain in the back
- Pain spreading from the back towards the arms and/or legs
- Trouble urinating
- Change in bowel habits
- Difficulty walking
- Delay in reaching growth and development milestones such as sitting, walking, and/or talking
If you are concerned that your child is displaying these or other unusual symptoms, it is important that you take him or her to your pediatrician right away. Spinal cord tumors in children are very rare, and in many cases these or other symptoms may be caused by a simple childhood illness. However, if your child’s pediatrician suspects the presence of a tumor, he or she will refer you to a neurologist and/or an oncologist for additional testing to ensure a prompt and accurate diagnosis.
Diagnostic Testing for Spinal Cord Tumors
Usually, the process of detecting and diagnosing a spinal cord tumor in children requires several steps:
- A physical exam and medical history: this will involve a discussion of your child’s general health and past health concerns and a physical exam to look for visible signs of disease such as a lump
- A neurological exam: this will check your child’s mental status, coordination, and ability to walk, talk, and function normally. It may involve a series of questions and/or physical tests—depending on the age and developmental status of the child—to check brain, nerve, and spinal cord function.
- Imaging exam: Physical and neurological exams will help determine if there is a health risk but will not provide any accurate diagnosis. In most cases, your child’s neurologist or oncologist will follow up all neurological exams with an imaging exam, which is the first step in detecting and locating an actual tumor. The most common imaging test is an MRI with gadolinium (also called nuclear magnetic resonance imaging). When injected near the site of the suspected tumor, the gadolinium collects near the abnormal cells, causing them to show up brighter in the image.
- Blood tests: Along with imaging tests, blood tests can indicate the presence of “tumor markers”, or abnormal substances in the blood caused by certain types of cancers.
Whenever possible, final diagnosis will occur during and after surgery to remove all or part of the spinal cord tumor. The goal of surgery is to remove all of the tumor, or as much of it as possible. A pathologist will then examine a piece of the tumor under a microscope to diagnose the type and grade of the tumor. This diagnosis will determine the course of follow-up treatment to kill any remaining tumorous cells and hopefully prevent the tumor from re-growing.
In some cases, however, the tumor may be growing in an area of the spinal cord where it cannot be removed surgically without causing excess damage to nearby healthy tissue. In these cases, diagnosis will be made based on imaging alone, and a non-surgical course of treatment will be determined based on that diagnosis.
More about Childhood Spinal Cord Tumor Cancers:
- About Childhood Spinal Cord Tumor Cancer – Detection and Diagnosis
- Causes, Risk Factors, and Prevention of Childhood Spinal Cord Tumor Cancer
- What are the signs and symptoms of Childhood Spinal Cord Tumor Cancer?
- Spinal Cord Tumor Cancer Treatment
- Spinal Cord Tumor Cancer – Stages and Prognosis
- What is the expected life span of Childhood Spinal Cord Tumor Cancer?
- After Treatment – Living as a Childhood Spinal Cord Tumor Cancer Survivor
Learn More About the Different Types of Childhood Cancers:
- Childhood Brain Tumor Cancer (Brain Stem Tumors)
- Spinal Cord Tumor Cancer
- Childhood Neuroblastoma Cancers
- Childhood Hodgkin Lymphoma Cancers
- Non-Hodgkin Lymphoma Cancers
- Wilms tumor (Kidney Tumors)
- Rhabdomyosarcoma
- Retinoblastoma
- Bone cancer (including osteosarcoma and Ewing sarcoma)
- Leukemia Cancers: Acute lymphocytic (lymphoblastic) leukemia (ALL) Acute myelogenous leukemia (AML); Juvenile myelomonocytic leukemia (JMML)
- Hepatoblastoma (Liver Cancer)
- Rhabdoid Tumors
About American Childhood Cancer Organization
American Childhood Cancer Organization (ACCO) is a non-profit charity dedicated to helping kids with cancer and their families navigate the difficult journey from cancer diagnosis through survivorship. Internationally, ACCO is the sole U.S. member of Childhood Cancer International (CCI), the largest patient-support organization for childhood cancer in the world. Here in the United States, ACCO promotes the critical importance of ensuring continued funding into new and better treatment protocols for childhood cancer. And most importantly, ACCO is focused on the children: developing and providing educational tools for children fighting cancer and their families, empowering them in their understanding of childhood cancer and the medical decisions they must make during this difficult journey. All of ACCO’s resources are available free of charge for families coping with childhood cancer.
For additional information about childhood cancer or on the ACCO, or to order resources for you or your child, please visit our website at www.acco.org , call 855.858.2226 or visit:

 Baseball season started in March of 2018 and Damon came home one day after practice saying that his right knee felt like his left one previously. They didn’t really think anything of it – so Damon finished out the baseball season the best he could. Damon’s mother, Tiffiney said, “for a minute the world stopped and went dark. It was Damon’s 16th birthday. It was something that we were somewhat prepared for thanks in part to our spor
Baseball season started in March of 2018 and Damon came home one day after practice saying that his right knee felt like his left one previously. They didn’t really think anything of it – so Damon finished out the baseball season the best he could. Damon’s mother, Tiffiney said, “for a minute the world stopped and went dark. It was Damon’s 16th birthday. It was something that we were somewhat prepared for thanks in part to our spor


 The central nervous system—including the brain and the spinal cord—grows and develops very quickly during childhood. This rapid rate of growth and development can make treating a brain and/or spinal cord tumor in children especially complicated for several reasons. First, the growth of the tumor can more easily damage the rapidly-changing tissues of the central nervous system (CNS). Second, the tissues of the CNS are extremely sensitive to the potentially damaging impact of chemotherapy, radiation, and other tools required to eliminate the tumor. These two issues are especially concerning when discussing survivorship issues for childhood brain and spinal cord tumors, and may have repercussions well into adulthood.
The central nervous system—including the brain and the spinal cord—grows and develops very quickly during childhood. This rapid rate of growth and development can make treating a brain and/or spinal cord tumor in children especially complicated for several reasons. First, the growth of the tumor can more easily damage the rapidly-changing tissues of the central nervous system (CNS). Second, the tissues of the CNS are extremely sensitive to the potentially damaging impact of chemotherapy, radiation, and other tools required to eliminate the tumor. These two issues are especially concerning when discussing survivorship issues for childhood brain and spinal cord tumors, and may have repercussions well into adulthood.
 By August, Kirby was completely paralyzed from the waist down. The doctors wouldn’t listen. Kirby’s parents decided to take matters into their own hands and took Kirby to a larger hospital to go through more tests. After a tearful meeting with one doctor expressing she didn’t know what was wrong with Kirby, they ordered an MRI. Moments after the MRI was read, the doctor told Sonnie, “we found out what is wrong with your son, he has tumors on his spine and they are spreading. It’s cancer. We need to get him on an airplane on our way to Children’s Hospital.” By noon, the family was on an airplane to Children’s Hospital of Colorado – a home to the Sargent family for the next six months.
By August, Kirby was completely paralyzed from the waist down. The doctors wouldn’t listen. Kirby’s parents decided to take matters into their own hands and took Kirby to a larger hospital to go through more tests. After a tearful meeting with one doctor expressing she didn’t know what was wrong with Kirby, they ordered an MRI. Moments after the MRI was read, the doctor told Sonnie, “we found out what is wrong with your son, he has tumors on his spine and they are spreading. It’s cancer. We need to get him on an airplane on our way to Children’s Hospital.” By noon, the family was on an airplane to Children’s Hospital of Colorado – a home to the Sargent family for the next six months.


 What are the key prognosis factors for childhood brain tumors?
What are the key prognosis factors for childhood brain tumors? When classed together in a single grouping, cancers in the brain and spinal cord are the second most common type of childhood cancer after leukemia. Brain and spinal cord tumors account for about 25% of all childhood cancer diagnoses, with more than 4,000 new cases diagnosed every year in the United States. In reality, however, it can be difficult to discuss “brain tumors” in general terms: oncologists recognize at least nine different sub-classifications of brain tumors in children, such as brain stem gliomas and ependymomas for example, with still more sub-groupings within those broad classifications.
When classed together in a single grouping, cancers in the brain and spinal cord are the second most common type of childhood cancer after leukemia. Brain and spinal cord tumors account for about 25% of all childhood cancer diagnoses, with more than 4,000 new cases diagnosed every year in the United States. In reality, however, it can be difficult to discuss “brain tumors” in general terms: oncologists recognize at least nine different sub-classifications of brain tumors in children, such as brain stem gliomas and ependymomas for example, with still more sub-groupings within those broad classifications.

 Grace loves to be crafty; she made a sign for the children to sign and date which says “Last Day of Chemo.” Throughout her treatment, she decided to paint pictures to brighten the nurses and the children’s days. When losing her hair became a reality, Grace decided to throw a party and shave her head. Grace’s brother and her best friend joined her in shaving their heads as well.
Grace loves to be crafty; she made a sign for the children to sign and date which says “Last Day of Chemo.” Throughout her treatment, she decided to paint pictures to brighten the nurses and the children’s days. When losing her hair became a reality, Grace decided to throw a party and shave her head. Grace’s brother and her best friend joined her in shaving their heads as well. lking to people about this part of her journey and is focused on helping others. Grace plans on learning more about oncology. She is excited for the future and can’t wait for her hair to start growing back!
lking to people about this part of her journey and is focused on helping others. Grace plans on learning more about oncology. She is excited for the future and can’t wait for her hair to start growing back! 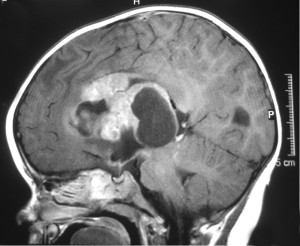 Any time a child is diagnosed with a brain tumor or other type of cancer, the most obvious question many parents ask is “why”. What caused this child to develop a brain tumor? Unfortunately, there is no easy answer to this question. Scientists now believe that the vast majority of brain tumors in children are the result of random gene mutations but have no satisfying answer as to why a particular gene mutation occurred or why it led to the growth of a brain tumor.
Any time a child is diagnosed with a brain tumor or other type of cancer, the most obvious question many parents ask is “why”. What caused this child to develop a brain tumor? Unfortunately, there is no easy answer to this question. Scientists now believe that the vast majority of brain tumors in children are the result of random gene mutations but have no satisfying answer as to why a particular gene mutation occurred or why it led to the growth of a brain tumor. After leukemia, brain tumors (including spinal cord tumors) are the second-most common type of cancer in children, accounting for about 25% of all childhood cancer diagnoses. Brain tumors begin within the delicate and complicated tissues of the brain or the cerebrospinal fluid (as well as the spinal cord or central nervous system, as these tumors are usually classed with brain tumors in children). When dealing with brain tumors in children, oncologists rarely differentiate between benign (non-cancerous) or malignant (cancerous) tumors; all tumors in the brain can be life-threatening whether technically cancerous or not. Instead, oncologists usually focus on how fast the tumor is growing, how quickly or easily it may spread throughout the brain or spinal cord, and how easy the tumor is to remove completely.
After leukemia, brain tumors (including spinal cord tumors) are the second-most common type of cancer in children, accounting for about 25% of all childhood cancer diagnoses. Brain tumors begin within the delicate and complicated tissues of the brain or the cerebrospinal fluid (as well as the spinal cord or central nervous system, as these tumors are usually classed with brain tumors in children). When dealing with brain tumors in children, oncologists rarely differentiate between benign (non-cancerous) or malignant (cancerous) tumors; all tumors in the brain can be life-threatening whether technically cancerous or not. Instead, oncologists usually focus on how fast the tumor is growing, how quickly or easily it may spread throughout the brain or spinal cord, and how easy the tumor is to remove completely. Meet Pedro, a 5-year-old warrior turning 6 this December. Pedro is one of three children in the Curiel family and is suffering from T Cell Acute Lymphoblastic leukemia (ALL). He is receiving delayed intensification treatments in California with his mom and siblings by his side.
Meet Pedro, a 5-year-old warrior turning 6 this December. Pedro is one of three children in the Curiel family and is suffering from T Cell Acute Lymphoblastic leukemia (ALL). He is receiving delayed intensification treatments in California with his mom and siblings by his side.  When he’s not receiving treatment, he is found drawing treasure maps around the house. Vilma said that he loves to draw these maps and hide his “treasure” and have his two brothers go find it! He started homeschooling in August, and he can now read a full sentence. He is expected to return to school after flu season.
When he’s not receiving treatment, he is found drawing treasure maps around the house. Vilma said that he loves to draw these maps and hide his “treasure” and have his two brothers go find it! He started homeschooling in August, and he can now read a full sentence. He is expected to return to school after flu season.