


Meet Eva, a forever 7 year old medulloblastoma warrior. Eva was a girly girl who always had her nails painted, loved playing with her brother Paddy and lived for ‘smuddles,’ a hug and squeeze from the ones she loved.
Eva was co-raised by her aunt, Tracy and her grandmother, Geraldine along with Tracy’s husband, Alan and brother, Paddy.
When Eva started to become agitated and lose her appetite, her family took note. When her uncle got married, Eva was very quiet which was very uncharacteristic of her normal sassy self. Two weeks later, Eva experienced a seizure while drinking milk. The seizure caused her to be unaware of her surroundings or her family in the room. When Geraldine called the doctor, they suggested just giving her an over the counter ear infection medication and said if things progressed to take her to the ER. Thankfully, they were able to fit her in on the same day and checked her ears. Eva was sent home with pain relief medicine.
Days before she was diagnosed, Eva started walking funny around the house and complaining of neck pain. She started demonstrating a head tilt and after many months of complaints and doctors visits, Tracy took matters into her own hands. After Eva had another seizure, Tracy took Eva back to the office and demanded to see a different doctor. This time, the doctor looked into Eva’s eyes and knew something was wrong. She excused herself from the room and called the emergency room to tell them she had a patient coming down with either a viral brain infection or medulloblastoma. The doctor noticed a very heavy buildup of fluid behind her eyes which was alarming. When the doctor came back into the room, she told the family she suspected it was a viral brain infection and that she needed an intravenous antibiotic. The doctor sent Eva in for an MRI and on October 3, 2012, Eva was diagnosed with stage 4 anaplastic medulloblastoma.
At the time of diagnosis, the doctors said they found a “mass” on Eva’s brain. The thought of “cancer” never entered Tracy’s brain and she thought it was benign. “They told us there was a mass on her brain. And you know what’s really funny about that time is when they said there was a mass on her brain, I still didn’t think it was cancer. I genuinely didn’t even know that children get cancer, isn’t that ridiculous?”
Five days after diagnosis, Eva had brain surgery to remove the golf ball size tumor. During her surgery, doctors noticed that the tumor had spread around her head and down her spine which they couldn’t touch. She was considered to be stage four at that time and was given a 30% chance of survival. During her 12 hour operation, Eva needed a blood transfusion and was watched a few days afterwards to see if she needed a shunt placed. Unfortunately she developed an infection in her brain and recovered quickly.
Eva was the second child in Ireland to receive the Milan protocol for the aggressive treatment of medulloblastoma. From reports, it was promised to give great results. She received a total of 12 months of chemotherapy, 6 weeks of radiotherapy twice daily and two stem cell transplants. As a result of treatment, she had nerve damage that would ultimately confine Eva to a wheelchair.
In June 2013, active treatment was complete and Eva was considered to have no evidence of disease. The next month however, Eva started to fall for no reason. Tracy called the oncologist who brought her in for another MRI. Another mass was found on her brain but not in the same spot. They found three particles but doctors did not think it was cancer. By October of 2013, Eva was unable to walk. She had lost all function and reverted into a baby. She had no control over her body, wore diapers and could not feed herself. Eva was still mentally and intellectually a four year old but unable to control her body.
When Eva lost her hair she looked at Tracy, gasped and said “look Trace, can you put that back in?!” Tracy took the hair and hid it behind her back and told her a “tall tale” about how some boys and girls hair go on a special adventure and that Eva’s hair is going on an adventure of its own which sparked an idea in Tracy. From then on, she’d tell Eva silly tales of adventures that “Hair” would go on, which became a character in their household.
Eva’s dream was to meet a princess, specifically Cinderella and for her Make-a-Wish, she was able to meet Cinderella in Disneyland in Paris. When she finally met Cinderella, Eva was completely speechless and in “awe” of her. That evening, the family was even able to have a dinner with Cinderella.
After missing so much school, Tracy decided to send Eva to a specialized school which would help with inhouse physical and occupational therapy among other specialized treatments. The school was almost 60 miles away but Eva loved it. She enjoyed the bus ride and would tell her family about her adventures every day. She would get her aide to help her play pranks on the principal and give silly nicknames to the bus driver.
Eva was put into a program at Stoke Mandeville hospital which helped her spine and brain. The family changed their life completely by changing their eating habits and supporting her immune system with the most natural ingredients. She seemed to be making good progress and even learned to feed herself again. At this time, Eva was even able to stand for 20 minutes with a standing frame.
In October 2015, Eva had seemed agitated again and by the end of October she complained of a sore neck again. She would cry at the drop of a hat and did not seem like she was in a good place. At her next doctor’s appointment, Tracy told the oncologist about her neck pain and was encouraged to wait for an upcoming MRI. Eva’s family was already aware that if she had a relapse that there was no more treatment available to her and if the treatment didn’t work, the options were to participate in a trial or to simply do nothing.
“In that entire three year period this was the only appointment I could not go to. I could not hear what the guy would say, so I sent my husband. I knew in my gut that something was wrong. I texted my husband throughout the day asking for updates. Now looking back, it was a coy way of saying nothing, but to me – it looked like hope and I took it. He responded with ‘all was well, the doctor wanted to see her again and we are on our way home’ and I didn’t think anything of it” said Tracy.
The oncologist said that there was a new trial that had existed however he felt that Eva had enough treatment and suggested morphine. Heartbroken, Tracy and her family decided to bring Eva home and keep her out of school in the middle of November. Unfortunately, Eva gained her angel wings in November of 2015.
 Eva’s legacy lives on in the series, “Eva’s Adventures,” which is Tracy’s passion project. She wanted her legacy of helping people to live on and has gone on to open up a charity of her very own and a park which features a “smuddle” park bench. They have held various fundraisers which has enabled the family to donate funds to other families in need and for cancer research in Ireland.
Eva’s legacy lives on in the series, “Eva’s Adventures,” which is Tracy’s passion project. She wanted her legacy of helping people to live on and has gone on to open up a charity of her very own and a park which features a “smuddle” park bench. They have held various fundraisers which has enabled the family to donate funds to other families in need and for cancer research in Ireland.
It should be noted that in late 2014 the oncologist that initially introduced Eva into the Milan protocol presented Eva’s case at a conference. He met several other doctors that had the same experiences with the treatment. Since then, the Milan protocol is not being utilized in Ireland.
Follow Eva’s Adventures and Tracy on social media below.
- FB: @EvasAdventure
- IG: @evasadventures_
- TW: @EvasAdventures
Learn more about Medulloblastoma by clicking here.
Together, we can make a difference.
Donate today… because kids can’t fight cancer alone®.



 David was brought into the PICU almost immediately where they met the oncologist who advised David and Elizabeth about David Jr.’s condition, DIPG. Diffuse Intrinsic Pontine Glioma (DIPG) remains one of the deadliest forms of childhood cancer, with a long-term survival rate of less than 1%. After receiving the diagnosis from the oncologist, David’s parents decided they wanted to get a biopsy even though that was against the head of pediatric neurosurgery. They were advised that having the biopsy would not change the result and a cure didn’t currently exist.
David was brought into the PICU almost immediately where they met the oncologist who advised David and Elizabeth about David Jr.’s condition, DIPG. Diffuse Intrinsic Pontine Glioma (DIPG) remains one of the deadliest forms of childhood cancer, with a long-term survival rate of less than 1%. After receiving the diagnosis from the oncologist, David’s parents decided they wanted to get a biopsy even though that was against the head of pediatric neurosurgery. They were advised that having the biopsy would not change the result and a cure didn’t currently exist. swallow to talking like normal, walking normally and getting around with no assistance!
swallow to talking like normal, walking normally and getting around with no assistance!



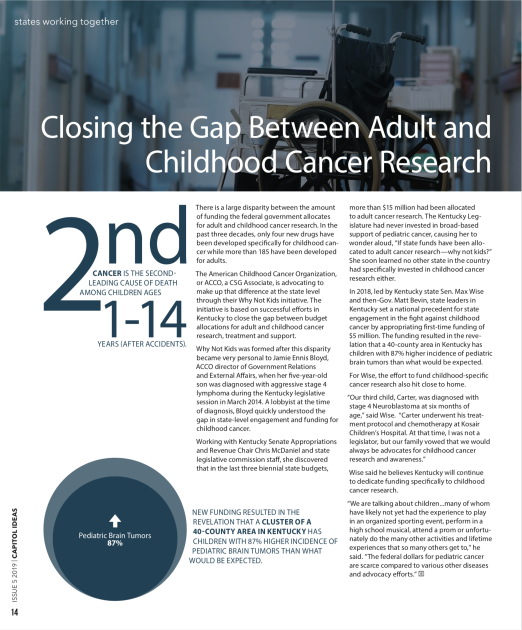
 After leukemia, brain tumors (including spinal cord tumors) are the second-most common type of cancer in children, accounting for about 25% of all childhood cancer diagnoses. Brain tumors begin within the delicate and complicated tissues of the brain or the cerebrospinal fluid (as well as the spinal cord or central nervous system, as these tumors are usually classed with brain tumors in children). When dealing with brain tumors in children, oncologists rarely differentiate between benign (non-cancerous) or malignant (cancerous) tumors; all tumors in the brain can be life-threatening whether technically cancerous or not. Instead, oncologists usually focus on how fast the tumor is growing, how quickly or easily it may spread throughout the brain or spinal cord, and how easy the tumor is to remove completely.
After leukemia, brain tumors (including spinal cord tumors) are the second-most common type of cancer in children, accounting for about 25% of all childhood cancer diagnoses. Brain tumors begin within the delicate and complicated tissues of the brain or the cerebrospinal fluid (as well as the spinal cord or central nervous system, as these tumors are usually classed with brain tumors in children). When dealing with brain tumors in children, oncologists rarely differentiate between benign (non-cancerous) or malignant (cancerous) tumors; all tumors in the brain can be life-threatening whether technically cancerous or not. Instead, oncologists usually focus on how fast the tumor is growing, how quickly or easily it may spread throughout the brain or spinal cord, and how easy the tumor is to remove completely.