ACCO is bringing back the name block shirts! We’ll have a fresh new design to share with you soon! These shirts carry the names, submitted by our community, of childhood cancer fighters: those who survived, those still fighting, and those no longer with us. Name submissions for 2024 are closed.
Shirts will be available May 1!
WAK Research & Advocacy Symposium
Healthcare professionals, legislators, and people who were personally touched by childhood cancer will all be under one roof at this Symposium. This activity will provide AMA PRA Category 1 credits™ and continuing education through Norton Healthcare.
If you can’t donate directly to ACCO, don’t worry! There are many other ways to financially contribute. You can host fundraisers, donate your old vehicle, or even just shop like you normally do at locations that donate to ACCO. Click the links below to learn more about different ways to give.
If you can’t donate directly to ACCO, don’t worry! There are many other ways to financially contribute. You can host fundraisers, donate your old vehicle, or even just shop like you normally do at locations that donate to ACCO. Click the links below to learn more about different ways to give.
Annika was diagnosed with neuroblastoma at just 10 weeks of age and has been fighting cancer for more than 6 years. Childhood cancer can make children and families feel like they are all alone, especially when low immunity means isolation to stay safe from life-threatening germs and viruses. Learn more about Annika and how the ACCO + Amazon is making a difference to ensure no child fights cancer alone.
Help support kids like Annika by raising awareness through signature programs like PJammin. Pajamas are the battle uniform for children with cancer. Too often it is a lonely battle fought isolated in hospital rooms or confined to staying at home for months – even years at a time. Help us let them know they are not alone.
Large scale change starts at the most local level. Founding Hope empowers individuals to turn compassion into action and engage their...
Founding Hope®
Pajamas are the battle uniform for children fighting cancer who often spend years living in their pajamas during treatment and recovery...
Our Heroes
For every day in September, we are inviting children who have been affected by cancer to explore their... interests in STEM
Get Involved
For every day in September, we are inviting children who have been affected by cancer to explore their... interests in STEM
What You Should Know
ACCO’s network of local divisions provide on-the-ground emotional, financial, and other critical support to families coping with childhood...
Latest News
February 15th is International Childhood Cancer Day! We commemorate this event with a very special tee shirt bearing the names of over 1,400 children...
Sorry, no posts matched your criteria.
Welcome to ACCO Fighting for Nearly 50 Years for Childhood Cancer
Our mission
We are a community of families, survivors, and friends who have been affected by childhood and adolescent cancer. We offer our community support, information, advocacy. We are their voice.
Childhood cancer is the #1 disease-related cause of death for children in the United States and many other countries. For those who survive, two-thirds will also endure chronic health conditions from the toxic side effects of cancer treatment, including secondary cancers and other life-threatening illnesses.
Through a new collaboration, the American Childhood Cancer Organization and Amazon are celebrating children diagnosed with cancer who demonstrate an interest in STEM. During September, Childhood Cancer Awareness Month, ACCO and Amazon will deliver smiles to 30 children in 30 days, one for every day of the month, through exciting STEM-related immersion experiences across the country. On behalf of each child, Amazon will also make donations to pediatric oncology programs across America committed to saving their lives.
Since 2008, ACCO’s partner Jel Sert has played a vital role bringing happiness to children with cancer, while simultaneously promoting our Gold Ribbon Awareness Program. Knowing the relief and joy an icy treat can bring, especially for children in treatment, Jel Sert generously provides pediatric cancer hospitals with a continuous supply of Fla-Vor-Ice freezer pops in a freezer decorated with the Gold Ribbon.
The American Childhood Cancer Organization (ACCO) would like to thank our partner – Microsoft Corporation – for hosting an incredible PJammin® for Kids with Cancer fundraising event!
YouCaring’s Compassionate Crowdfunding™ program helps families facing financial hardship due to childhood cancer to develop and coordinate a personalized online fundraising campaign. YouCaring’s revolutionary crowdfunding techniques are designed to walk you through the fundraising process, with no additional fees, so you can ease your financial burden and focus on what really matters: helping your child beat this terrible disease!
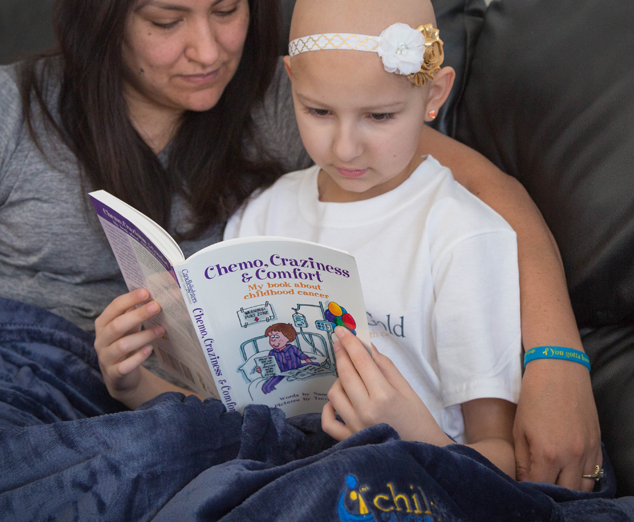
In an effort to raise awareness and help families of children undergoing cancer treatments, La Roche-Posay is proud to partner with the American Childhood Cancer Organization. To help facilitate communication between children undergoing treatment and their loved ones, La Roche-Posay will donate kits with emotive tools designed to help kids express their feelings. In addition, La Roche-Posay will also host a “donations” button on their website for customers to donate directly to ACCO.
PALMCo makes it easy: for every customer that registers with PALMCo and its sister company, Columbia Utilities, PALMco pledges a $1.00 donation every month to support the ACCO’s critical mission to offer resources, information, and support to children and families impacted by cancer. Once you have registered, all you need to do is pay your utility bill every month and you are joining the fight against childhood cancer.
Goorin Bros. Hats Company has generously donated a selection of high-quality hats for children and teens fighting childhood cancer. If you would like a hat to brighten the spirits of your warrior, use the discount code 'FREE HAT' when you visit the ACCO store.
The Loft Entertainment is a celebrity marketing and brand acceleration company that is the "go to" company matchmaking celebrities and Influencers to brands specializing in the areas of celebrity marketing, brand acceleration, content creation, and so much more. In September 2018, The Loft + ACCO will challenge their key Influencers in an online campaign to donate #OneGoodDollar to raise awareness and program funding for ACCO.
Matilda Jane
Denise Demarchis, founder of the Matilda Jane Clothing (MJC) line said, "It's all about keeping a little girl... a little girl. Keeping her youthful. Keeping her spinning and twirling and carefree. And most importantly, bringing her happiness." Denise passed away from cancer, but true to her legacy, MJC is now bringing happiness to little girls fighting cancer too. In September 2018, we are proud to unveil a GO GOLD Matilda Jane Platinum dress celebrating the bravery of little girls battling cancer and their desire to still express their girly-ness, even after losing their hair. Designed by two cancer moms, the Bennett dress features gold fabric and gold glitter ribbon - showcasing the gold ribbon as the international symbol of childhood cancer - as well as additional ruffles and pink lace for an extra helping of girly sweetness. Proceeds from purchase of the dress will benefit ACCO. To purchase the dress and to learn more visit www.matildajaneplatinum.com.
The American Childhood Cancer Organization (ACCO) is grateful for the support from Servier Pharmaceuticals – a U.S. subsidiary of the Servier Group, an international pharmaceutical company that is governed by a non-profit foundation. Servier Pharmaceutical’s drug pipeline includes Oncaspar® (pegaspargase) – a chemotherapy drug that is essential to the successful treatment of pediatric acute lymphoblastic leukemia (ALL). ACCO appreciates the support from Servier to aid in the expansion of our Why Not Kids and Founding Hope Programs and provide resources to execute essential programs and services that address the critical needs of children being treated for cancer.
Erimish and the American Childhood Cancer Organization began a partnership in September 2020 with a variety of custom bracelets inspired by the bravest childhood cancer warriors. With custom stacks and singles in adult and youth sizes, there is an option for everyone! Whether you choose to Go Gold® or rock the colorful option, you’ll be able to keep your favorite warrior close to you with each of these beautiful designs! Erimish is generously committed to donating 50% of each bracelet or stack sold to ACCO. To start shopping or learn more, click the button below and look for the “Warrior” designs.
Through a new collaboration, the American Childhood Cancer Organization and Amazon are celebrating children diagnosed with cancer who demonstrate an interest in STEM. During September, Childhood Cancer Awareness Month, ACCO and Amazon will deliver smiles to 30 children in 30 days, one for every day of the month, through exciting STEM-related immersion experiences across the country. On behalf of each child, Amazon will also make donations to pediatric oncology programs across America committed to saving their lives.
Since 2008, ACCO’s partner Jel Sert has played a vital role bringing happiness to children with cancer, while simultaneously promoting our Gold Ribbon Awareness Program. Knowing the relief and joy an icy treat can bring, especially for children in treatment, Jel Sert generously provides pediatric cancer hospitals with a continuous supply of Fla-Vor-Ice freezer pops in a freezer decorated with the Gold Ribbon.
The American Childhood Cancer Organization (ACCO) would like to thank our partner – Microsoft Corporation – for hosting an incredible PJammin® for Kids with Cancer fundraising event!
YouCaring’s Compassionate Crowdfunding™ program helps families facing financial hardship due to childhood cancer to develop and coordinate a personalized online fundraising campaign. YouCaring’s revolutionary crowdfunding techniques are designed to walk you through the fundraising process, with no additional fees, so you can ease your financial burden and focus on what really matters: helping your child beat this terrible disease!
In an effort to raise awareness and help families of children undergoing cancer treatments, La Roche-Posay is proud to partner with the American Childhood Cancer Organization. To help facilitate communication between children undergoing treatment and their loved ones, La Roche-Posay will donate kits with emotive tools designed to help kids express their feelings. In addition, La Roche-Posay will also host a “donations” button on their website for customers to donate directly to ACCO.
PALMCo makes it easy: for every customer that registers with PALMCo and its sister company, Columbia Utilities, PALMco pledges a $1.00 donation every month to support the ACCO’s critical mission to offer resources, information, and support to children and families impacted by cancer. Once you have registered, all you need to do is pay your utility bill every month and you are joining the fight against childhood cancer.
Goorin Bros. Hats Company has generously donated a selection of high-quality hats for children and teens fighting childhood cancer. If you would like a hat to brighten the spirits of your warrior, use the discount code 'FREE HAT' when you visit the ACCO store.
Through a new collaboration, the American Childhood Cancer Organization and Amazon are celebrating children diagnosed with cancer who demonstrate an interest in STEM. During September, Childhood Cancer Awareness Month, ACCO and Amazon will deliver smiles to 30 children in 30 days, one for every day of the month, through exciting STEM-related immersion experiences across the country. On behalf of each child, Amazon will also make donations to pediatric oncology programs across America committed to saving their lives.
Since 2008, ACCO’s partner Jel Sert has played a vital role bringing happiness to children with cancer, while simultaneously promoting our Gold Ribbon Awareness Program. Knowing the relief and joy an icy treat can bring, especially for children in treatment, Jel Sert generously provides pediatric cancer hospitals with a continuous supply of Fla-Vor-Ice freezer pops in a freezer decorated with the Gold Ribbon.
The American Childhood Cancer Organization (ACCO) would like to thank our partner – Microsoft Corporation – for hosting an incredible PJammin® for Kids with Cancer fundraising event!
YouCaring’s Compassionate Crowdfunding™ program helps families facing financial hardship due to childhood cancer to develop and coordinate a personalized online fundraising campaign. YouCaring’s revolutionary crowdfunding techniques are designed to walk you through the fundraising process, with no additional fees, so you can ease your financial burden and focus on what really matters: helping your child beat this terrible disease!
In an effort to raise awareness and help families of children undergoing cancer treatments, La Roche-Posay is proud to partner with the American Childhood Cancer Organization. To help facilitate communication between children undergoing treatment and their loved ones, La Roche-Posay will donate kits with emotive tools designed to help kids express their feelings. In addition, La Roche-Posay will also host a “donations” button on their website for customers to donate directly to ACCO.
PALMCo makes it easy: for every customer that registers with PALMCo and its sister company, Columbia Utilities, PALMco pledges a $1.00 donation every month to support the ACCO’s critical mission to offer resources, information, and support to children and families impacted by cancer. Once you have registered, all you need to do is pay your utility bill every month and you are joining the fight against childhood cancer.
Goorin Bros. Hats Company has generously donated a selection of high-quality hats for children and teens fighting childhood cancer. If you would like a hat to brighten the spirits of your warrior, use the discount code 'FREE HAT' when you visit the ACCO store.
Latest News Fighting for Nearly 50 Years for Childhoood Cancer
Latest News
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Duis id ultricies sapien. Mauris ac dapibus urna. In viverra placerat blandit. Proin eget eros nec metus posuere bibendum. Praesent ex lectus, euismod eget interdum non vestibulum ante porttitor in. Nullam et elementum leo.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Duis id ultricies sapien. Mauris ac dapibus urna. In viverra placerat blandit. Proin eget eros nec metus posuere bibendum. Praesent ex lectus, euismod eget interdum non vestibulum ante porttitor in. Nullam et elementum leo.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Duis id ultricies sapien. Mauris ac dapibus urna. In viverra placerat blandit. Proin eget eros nec metus posuere bibendum. Praesent ex lectus, euismod eget interdum non vestibulum ante porttitor in. Nullam et elementum leo.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Duis id ultricies sapien. Mauris ac dapibus urna. In viverra placerat blandit. Proin eget eros nec metus posuere bibendum. Praesent ex lectus, euismod eget interdum non vestibulum ante porttitor in. Nullam et elementum leo.