

Childhood Neuroblastoma: Treatment Options
 Neuroblastoma is a form of childhood cancer that begins in the early development of nerve cells. Because this rare form of cancer usually begins when the sympathetic nervous system is developing in an embryo or fetus, it occurs most often in infants and very young children, and is extremely rare in children over the age of 10. And because it begins when nerve cells are developing very quickly, the cancer’s development within each child can vary widely: some neuroblastomas grow and spread very quickly while other neuroblastomas grow very slowly. In some cases, the cancerous cells simply disappear on their own, while in other cases, the cancerous cells mature into normal nerve cells. Therefore, treatment for neuroblastoma often depends, upon other factors, on the stage and risk grouping of the cancer, as well as on the age of the child.
Neuroblastoma is a form of childhood cancer that begins in the early development of nerve cells. Because this rare form of cancer usually begins when the sympathetic nervous system is developing in an embryo or fetus, it occurs most often in infants and very young children, and is extremely rare in children over the age of 10. And because it begins when nerve cells are developing very quickly, the cancer’s development within each child can vary widely: some neuroblastomas grow and spread very quickly while other neuroblastomas grow very slowly. In some cases, the cancerous cells simply disappear on their own, while in other cases, the cancerous cells mature into normal nerve cells. Therefore, treatment for neuroblastoma often depends, upon other factors, on the stage and risk grouping of the cancer, as well as on the age of the child.
Treatment for Low Risk Neuroblastoma
Any time a child is diagnosed with cancer—neuroblastoma or otherwise—the goal is to utilize the least intensive treatment to minimize short- and long-term side effects while maximizing the damage to the cancerous cells. For children with low risk neuroblastoma, treatment may be as simple as frequent and routine monitoring to determine whether the tumor may die or mature into normal cells without intervention.
Surgery may be the only required treatment if all or most of the tumorous cells can be reached and safely removed. Even if it is not possible to remove the entire tumor with surgery, in some cases any remaining cancerous cells may die or mature on their own without the need for any additional intervention.
Chemotherapy may be required if the tumor cannot be safely or effectively removed with surgery or if the tumor continues to grow abnormally after surgery. If the tumor is causing symptoms due to its proximity to a nearby organ, a short course of chemotherapy may be utilized in advance of surgery to reduce the size of the tumor. A similar treatment method may be utilized to make the tumor more accessible to a surgeon.
Generally speaking, oncologists try to avoid the use of radiation therapy in young children due to the extremely high risk of negative short- and long-term side effects.
Treatment for Intermediate Risk Neuroblastoma
For children with intermediate risk neuroblastoma, treatment almost always involves a combination of surgery and chemotherapy. A typical course of treatment usually involves four to eight cycles of chemotherapy before and following surgery. One or more rounds of radiation therapy may be utilized only if the cancerous cells do not respond to chemotherapy or if the tumor is causing symptoms that require emergency treatment; again, the goal is to avoid the use of radiation therapy whenever possible in young children.
Treatment for High Risk Neuroblastoma
Children with high risk neuroblastoma will require aggressive treatment that usually involves an intensive mix of chemotherapy, surgery, radiation therapy, stem cell transplant(s), retinoid therapy, and immunotherapy.
Treatment usually starts with extremely aggressive chemotherapy designed to destroy as much of the cancer as possible, sometimes coupled with surgery to remove any remaining tumors. This phase of treatment is known as induction. If induction is successful, it will send the cancer into remission.
Induction is usually followed by a consolidation phase, which involves additional intensive chemotherapy treatments to rid the body of any remaining cancerous cells. Because this phase of treatment often destroys normal bone marrow as well as the cancer, it usually involves one or more stem cell transplants to help the body replace the damaged bone marrow. Stem cell transplants may be followed by immunotherapy to help boost the body’s ability to find and destroy cancer cells on its own, as well as radiation therapy at the primary tumor site to prevent recurrence.
If induction is successful, treatment will move to a maintenance phase involving a combination of additional immunotherapy and retinoid therapy. Retinoids are a type of differentiating agent that is believed to help some types of cancer cells mature into normal cells. The goal of this phase of treatment is to reduce the risk of recurrent neuroblastoma.
More about Childhood Neuroblastoma Cancers:
- About Childhood Neuroblastoma Cancer – Detection and Diagnosis
- Causes, Risk Factors, and Prevention of Childhood Neuroblastoma Cancer
- What are the signs and symptoms of Childhood Neuroblastoma Cancer?
- Childhood Neuroblastoma Cancer Treatment
- Childhood Neuroblastoma Cancer – Stages and Prognosis
- What is the expected life span of Childhood Neuroblastoma Cancer?
- After Treatment – Living as a Childhood Neuroblastoma Cancer Survivor
Learn More About the Different Types of Childhood Cancers:
- Childhood Brain Tumor Cancer (Brain Stem Tumors)
- Spinal Cord Tumor Cancer
- Childhood Neuroblastoma Cancers
- Childhood Hodgkin Lymphoma Cancers
- Non-Hodgkin Lymphoma Cancers
- Wilms tumor (Kidney Tumors)
- Rhabdomyosarcoma
- Retinoblastoma
- Bone cancer (including osteosarcoma and Ewing sarcoma)
- Leukemia Cancers: Acute lymphocytic (lymphoblastic) leukemia (ALL) Acute myelogenous leukemia (AML); Juvenile myelomonocytic leukemia (JMML)
- Hepatoblastoma (Liver Cancer)
- Rhabdoid Tumors
Together, we can make a difference.
Donate today because kids can’t fight cancer alone®.

About American Childhood Cancer Organization
The American Childhood Cancer Organization was founded in 1970 by parents of children and adolescents diagnosed with cancer. As the nation’s oldest and largest grassroots organization dedicated to childhood cancer, ACCO is committed to shaping policy, supporting research, raising awareness, and providing free educational resources to kids with cancer, survivors, and their families. Additionally, ACCO is the sole U.S. member of Childhood Cancer International (CCI) and has helped support more than half a million families over the past 50 years. Help make childhood cancer a national health priority because kids can’t fight cancer alone®.
For more information about how ACCO can help your family, call 855.858.2226 or visit:
 The central nervous system (CNS) is composed of the brain and the spinal cord, a delicate and sensitive column of nerves protected by the boney vertebrae of the spine. Statistically, CNS cancers are all grouped together as “brain and spinal cord tumors”, but of course in reality, there are a number of different and distinct types of spinal cord tumors, and each specific tumor requires a unique treatment approach and carries its own outlook for long-term survivorship.
The central nervous system (CNS) is composed of the brain and the spinal cord, a delicate and sensitive column of nerves protected by the boney vertebrae of the spine. Statistically, CNS cancers are all grouped together as “brain and spinal cord tumors”, but of course in reality, there are a number of different and distinct types of spinal cord tumors, and each specific tumor requires a unique treatment approach and carries its own outlook for long-term survivorship.
 surgery. After reading the scans, doctors determined that her intestines and stomach were severely damaged but no holes were present saying that she
surgery. After reading the scans, doctors determined that her intestines and stomach were severely damaged but no holes were present saying that she 

 When classifying childhood cancers and discussing important statistics, tumors of the brain and tumors of the spinal cord are often lumped together as one broad grouping (although, of course, when diagnosing childhood cancer, each tumor is specified as a more specific “type”). And in general, treatment options for both spinal cord tumors and brain tumors are the same, usually consisting of some combination of
When classifying childhood cancers and discussing important statistics, tumors of the brain and tumors of the spinal cord are often lumped together as one broad grouping (although, of course, when diagnosing childhood cancer, each tumor is specified as a more specific “type”). And in general, treatment options for both spinal cord tumors and brain tumors are the same, usually consisting of some combination of Meet Emma…
Meet Emma…
 In the span of ten minutes, Emma’s life changed forever. Megan said that the doctor said, “we see a mass, she is being flown to Oklahoma City.” It took a few minutes before I could catch my breath. I held Emma’s hand and I told her straight up. “Emma, the doctors say they see a tumor and we have to fly to Oklahoma City for another doctor to look at you.” Emma said, “Momma, I will be your angel, and when it is time for you to come, I will come get you.” Heartbreaking.
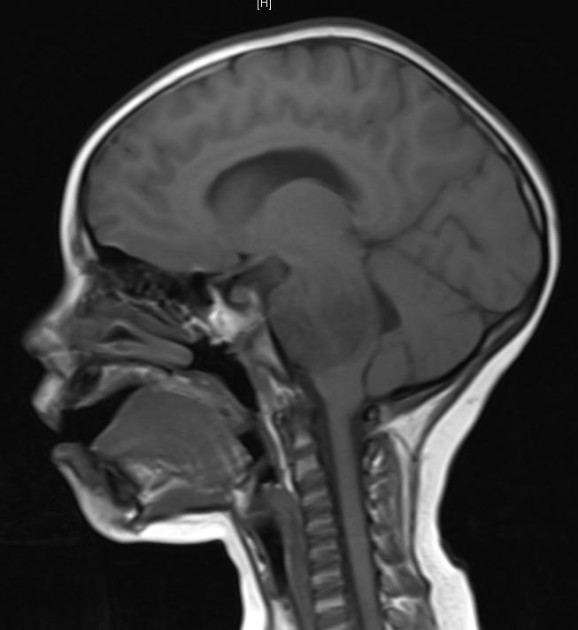
In the span of ten minutes, Emma’s life changed forever. Megan said that the doctor said, “we see a mass, she is being flown to Oklahoma City.” It took a few minutes before I could catch my breath. I held Emma’s hand and I told her straight up. “Emma, the doctors say they see a tumor and we have to fly to Oklahoma City for another doctor to look at you.” Emma said, “Momma, I will be your angel, and when it is time for you to come, I will come get you.” Heartbreaking. an MRI was performed two days later. The next day, the tumor was removed during her craniotomy. After a preliminary diagnosis of medulloblastoma that was believed to be cancerous, it was confirmed two days later. Treatment has consisted of a port placement, 30 proton therapy treatments, lumbar puncture, chemotherapy, MRI’s of the spine and head under general anesthesia, bone targeted therapies (BTT), bilateral tubes, and multiple hospitalizations. Since Emma’s tumor is so rare, she is currently in a trial where she gets 25% less chemo and proton therapy doses. She’s the only one participating in this study because of the rarity of the tumor. Her results will help to change the way cancer is treated.
an MRI was performed two days later. The next day, the tumor was removed during her craniotomy. After a preliminary diagnosis of medulloblastoma that was believed to be cancerous, it was confirmed two days later. Treatment has consisted of a port placement, 30 proton therapy treatments, lumbar puncture, chemotherapy, MRI’s of the spine and head under general anesthesia, bone targeted therapies (BTT), bilateral tubes, and multiple hospitalizations. Since Emma’s tumor is so rare, she is currently in a trial where she gets 25% less chemo and proton therapy doses. She’s the only one participating in this study because of the rarity of the tumor. Her results will help to change the way cancer is treated. As a result of her diagnosis, Emma suffers from anxiety and depression, decreased fine motor skills and complete left sided deafness. However, Megan says, “She has finally embraced beauty and that it comes in lots of different ways. She is funny and spirited – and yet will lay in my lap and cry often at night.” Emma can be described as ornery, witty and a quick thinker – and her mom wouldn’t have it any other way.
As a result of her diagnosis, Emma suffers from anxiety and depression, decreased fine motor skills and complete left sided deafness. However, Megan says, “She has finally embraced beauty and that it comes in lots of different ways. She is funny and spirited – and yet will lay in my lap and cry often at night.” Emma can be described as ornery, witty and a quick thinker – and her mom wouldn’t have it any other way. and Amazon + ACCO’s 2018 Ambassador Grace Eline was in the Gallery for the State of the Union speech as an Honored Guest of the President and First Lady.
and Amazon + ACCO’s 2018 Ambassador Grace Eline was in the Gallery for the State of the Union speech as an Honored Guest of the President and First Lady. Beginning in early 2019, our team at ACCO has had several positive and productive meetings with the top leadership at the Department of Health and Human Services (HHS), including HHS Secretary Alex Azar and HHS Assistant Secretary for Health Dr. Brett Giroir. These discussions were unique opportunities to provide decision makers with critical data gathered from our work across the country and around the world. We are grateful to the Administration for giving us a seat at the table and look forward to continuing to share insights and work together.
Beginning in early 2019, our team at ACCO has had several positive and productive meetings with the top leadership at the Department of Health and Human Services (HHS), including HHS Secretary Alex Azar and HHS Assistant Secretary for Health Dr. Brett Giroir. These discussions were unique opportunities to provide decision makers with critical data gathered from our work across the country and around the world. We are grateful to the Administration for giving us a seat at the table and look forward to continuing to share insights and work together.
 ACCO’s team attended Action Days in Washington alongside over 200 other childhood cancer advocates from across the country. In hundreds of meetings on Capitol Hill, Action Day advocates thanked Congress and the Trump Administration for making childhood cancer a national priority and urged them to keep up their important work to ensure full funding for efforts across the board to improve treatments and find cures. Specifically, we called on Members of Congress to fully fund: the National Institutes of Health (NIH) and NCI; the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which was passed into law last Summer; and the President’s Childhood Cancer Initiative.
ACCO’s team attended Action Days in Washington alongside over 200 other childhood cancer advocates from across the country. In hundreds of meetings on Capitol Hill, Action Day advocates thanked Congress and the Trump Administration for making childhood cancer a national priority and urged them to keep up their important work to ensure full funding for efforts across the board to improve treatments and find cures. Specifically, we called on Members of Congress to fully fund: the National Institutes of Health (NIH) and NCI; the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which was passed into law last Summer; and the President’s Childhood Cancer Initiative.
 Is staging relevant for childhood brain tumors? In fact, this is one of the major differences between brain tumors and other types of cancers in children. Regardless of whether they are malignant (cancerous) or benign (non-cancerous), brain tumors in children rarely spread to other organs beyond the central nervous system (which includes the brain and the spinal cord). Therefore, oncologists do not utilize a formal staging system when diagnosing and treating brain cancers.
Is staging relevant for childhood brain tumors? In fact, this is one of the major differences between brain tumors and other types of cancers in children. Regardless of whether they are malignant (cancerous) or benign (non-cancerous), brain tumors in children rarely spread to other organs beyond the central nervous system (which includes the brain and the spinal cord). Therefore, oncologists do not utilize a formal staging system when diagnosing and treating brain cancers. Meet Colton…
Meet Colton…
 According to Shannon, “radiation would only buy us time and there were trials we could participate in, but none were proven to save our child at this point.” During his treatment, Colton had multiple labs done, hospital stays, pneumonia, seizures and eventually lost his ability to walk, talk and swallow. He endured 30 rounds of radiation with a smile on his face. He also participated in a clinical trial for a year at Cincinnati Children’s Hospital.
According to Shannon, “radiation would only buy us time and there were trials we could participate in, but none were proven to save our child at this point.” During his treatment, Colton had multiple labs done, hospital stays, pneumonia, seizures and eventually lost his ability to walk, talk and swallow. He endured 30 rounds of radiation with a smile on his face. He also participated in a clinical trial for a year at Cincinnati Children’s Hospital. 
 The brain is the “command center” for our entire central nervous system, yet despite its critical role in every aspect of human life, it is one of the most delicate organs in the entire body. Any abnormal growth, or tumor, in the brain—whether technically malignant (cancerous) or benign (non-cancerous)—can cause serious damage to the healthy brain tissue and significantly impact the body’s ability to function normally. Therefore, treating a brain tumor requires taking into consideration
The brain is the “command center” for our entire central nervous system, yet despite its critical role in every aspect of human life, it is one of the most delicate organs in the entire body. Any abnormal growth, or tumor, in the brain—whether technically malignant (cancerous) or benign (non-cancerous)—can cause serious damage to the healthy brain tissue and significantly impact the body’s ability to function normally. Therefore, treating a brain tumor requires taking into consideration