

On February 5, 2019, President Trump announced funding for a new Childhood Cancer Initiative in the amount of $500 million over 10 years. Gold Ribbon Hero and Amazon + ACCO’s 2018 Ambassador Grace Eline was in the Gallery for the State of the Union speech as an Honored Guest of the President and First Lady.
and Amazon + ACCO’s 2018 Ambassador Grace Eline was in the Gallery for the State of the Union speech as an Honored Guest of the President and First Lady.
ACCO has been working to raise the profile of childhood cancer for 49 years and we were thrilled to see the President recognize this cause as a national priority.
Since the announcement, we have been working tirelessly to maintain momentum. We are continuing our longstanding leadership role in working with policymakers and agenda setters in Washington to bring the President’s initiative to fruition and to push forward other policy priorities for kids and families fighting cancer. Here are a few updates on our recent advocacy work. You can stay up-to-date on these efforts by signing up for our Advocacy newsletter.
On the Ground at HHS
 Beginning in early 2019, our team at ACCO has had several positive and productive meetings with the top leadership at the Department of Health and Human Services (HHS), including HHS Secretary Alex Azar and HHS Assistant Secretary for Health Dr. Brett Giroir. These discussions were unique opportunities to provide decision makers with critical data gathered from our work across the country and around the world. We are grateful to the Administration for giving us a seat at the table and look forward to continuing to share insights and work together.
Beginning in early 2019, our team at ACCO has had several positive and productive meetings with the top leadership at the Department of Health and Human Services (HHS), including HHS Secretary Alex Azar and HHS Assistant Secretary for Health Dr. Brett Giroir. These discussions were unique opportunities to provide decision makers with critical data gathered from our work across the country and around the world. We are grateful to the Administration for giving us a seat at the table and look forward to continuing to share insights and work together.
Early this month, we also participated with other childhood cancer advocacy organizations in a kick-off call with HHS and the National Cancer Institute (NCI) to open dialogue about plans for the President’s Childhood Cancer Initiative and its intended focus on broad-scale data sharing. We recognize this effort as an opportunity for the childhood cancer community to lead and will continue to participate in these important strategy discussions as the Initiative takes shape.
Grace Goes to Washington…Again!

Last week, ACCO Ambassador Grace Eline was again invited to the nation’s capital, this time to the White House for a round table discussion with Vice President Mike Pence and leadership from HHS and NCI. Grace and other young advocates shared their own experiences as cancer fighters and survivors and discussed the promise of the President’s Childhood Cancer Initiative. We are proud of Grace’s tireless efforts on behalf of all kids and are looking forward to supporting her and other ACCO Ambassadors and advocates as we work with the Administration to achieve the President’s pledge.
#FightCancerforKids at Action Days
 ACCO’s team attended Action Days in Washington alongside over 200 other childhood cancer advocates from across the country. In hundreds of meetings on Capitol Hill, Action Day advocates thanked Congress and the Trump Administration for making childhood cancer a national priority and urged them to keep up their important work to ensure full funding for efforts across the board to improve treatments and find cures. Specifically, we called on Members of Congress to fully fund: the National Institutes of Health (NIH) and NCI; the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which was passed into law last Summer; and the President’s Childhood Cancer Initiative.
ACCO’s team attended Action Days in Washington alongside over 200 other childhood cancer advocates from across the country. In hundreds of meetings on Capitol Hill, Action Day advocates thanked Congress and the Trump Administration for making childhood cancer a national priority and urged them to keep up their important work to ensure full funding for efforts across the board to improve treatments and find cures. Specifically, we called on Members of Congress to fully fund: the National Institutes of Health (NIH) and NCI; the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which was passed into law last Summer; and the President’s Childhood Cancer Initiative.
ACCO’s Global Commitment

In addition to ACCO’s leadership in the U.S., ACCO is also deeply engaged in childhood cancer advocacy at the global level. As a follow up to our participation as
invited speaker at the U.N. General Assembly’s side event on childhood cancer, we serve on the steering committee and working groups of the World Health Organization’s (WHO) Global Initiative on Childhood Cancer. In this capacity we are working to address the global survival disparity of children diagnosed with cancer, focusing on increasing access to essential medicines, supportive care, innovative research, patient and family education and making childhood cancer an international child health priority.
—
As the oldest and largest grassroots childhood cancer organization, and the only U.S. member of Childhood Cancer International, ACCO is dedicated to fighting cancer, the number one non-communicable disease killer of children in the U.S. We know that childhood cancer is a big problem that requires an even bigger effort to find a solution. That’s why we are pushing for progress all around the world and at every level.
To sign up for federal and state-level advocacy newsletters, click here.
Together, we can make a difference.
Donate today because kids can’t fight cancer alone®.

About American Childhood Cancer Organization
The American Childhood Cancer Organization was founded in 1970 by parents of children and adolescents diagnosed with cancer. As the nation’s oldest and largest grassroots organization dedicated to childhood cancer, ACCO is committed to shaping policy, supporting research, raising awareness, and providing free educational resources to kids with cancer, survivors, and their families. Additionally, ACCO is the sole U.S. member of Childhood Cancer International (CCI) and has helped support more than half a million families over the past 50 years. Help make childhood cancer a national health priority because kids can’t fight cancer alone®.
For more information about how ACCO can help your family, call 855.858.2226 or visit:
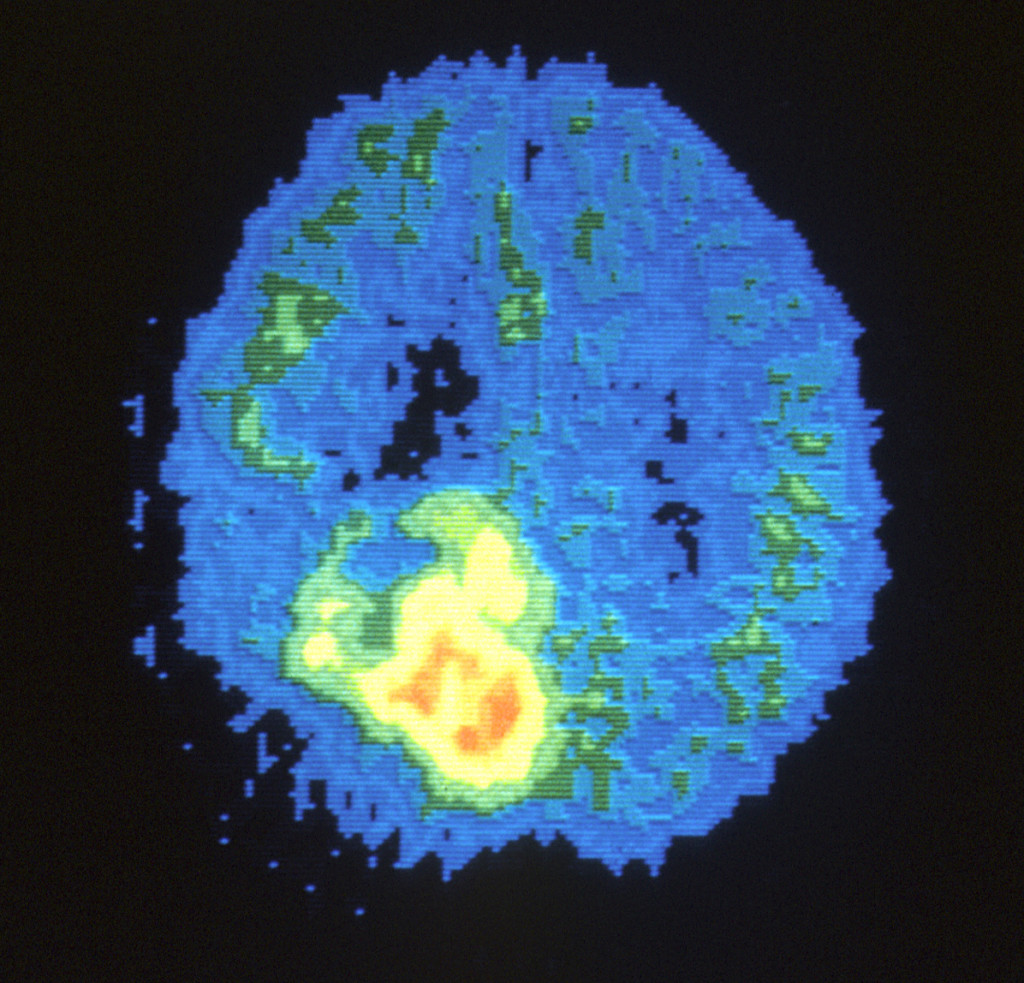
 Is staging relevant for childhood brain tumors? In fact, this is one of the major differences between brain tumors and other types of cancers in children. Regardless of whether they are malignant (cancerous) or benign (non-cancerous), brain tumors in children rarely spread to other organs beyond the central nervous system (which includes the brain and the spinal cord). Therefore, oncologists do not utilize a formal staging system when diagnosing and treating brain cancers.
Is staging relevant for childhood brain tumors? In fact, this is one of the major differences between brain tumors and other types of cancers in children. Regardless of whether they are malignant (cancerous) or benign (non-cancerous), brain tumors in children rarely spread to other organs beyond the central nervous system (which includes the brain and the spinal cord). Therefore, oncologists do not utilize a formal staging system when diagnosing and treating brain cancers. Meet Colton…
Meet Colton…
 According to Shannon, “radiation would only buy us time and there were trials we could participate in, but none were proven to save our child at this point.” During his treatment, Colton had multiple labs done, hospital stays, pneumonia, seizures and eventually lost his ability to walk, talk and swallow. He endured 30 rounds of radiation with a smile on his face. He also participated in a clinical trial for a year at Cincinnati Children’s Hospital.
According to Shannon, “radiation would only buy us time and there were trials we could participate in, but none were proven to save our child at this point.” During his treatment, Colton had multiple labs done, hospital stays, pneumonia, seizures and eventually lost his ability to walk, talk and swallow. He endured 30 rounds of radiation with a smile on his face. He also participated in a clinical trial for a year at Cincinnati Children’s Hospital. 
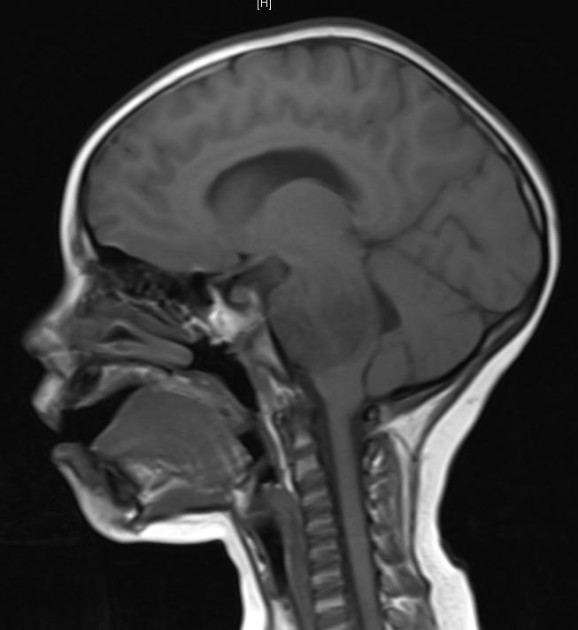
 The brain is the “command center” for our entire central nervous system, yet despite its critical role in every aspect of human life, it is one of the most delicate organs in the entire body. Any abnormal growth, or tumor, in the brain—whether technically malignant (cancerous) or benign (non-cancerous)—can cause serious damage to the healthy brain tissue and significantly impact the body’s ability to function normally. Therefore, treating a brain tumor requires taking into consideration
The brain is the “command center” for our entire central nervous system, yet despite its critical role in every aspect of human life, it is one of the most delicate organs in the entire body. Any abnormal growth, or tumor, in the brain—whether technically malignant (cancerous) or benign (non-cancerous)—can cause serious damage to the healthy brain tissue and significantly impact the body’s ability to function normally. Therefore, treating a brain tumor requires taking into consideration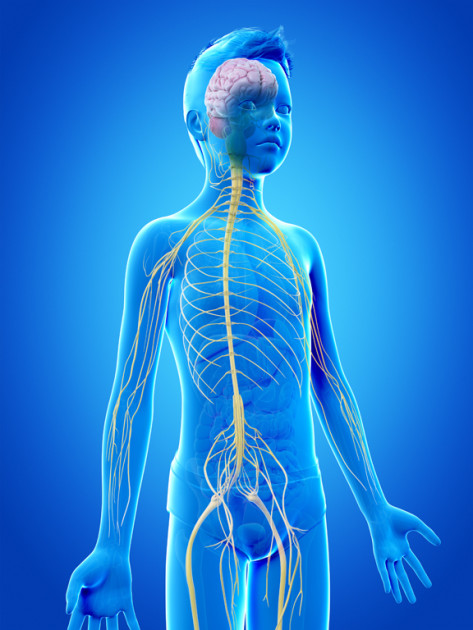 Taken together, the brain and the spinal cord make up what is known as the “central nervous system” (CNS). The CNS is responsible for our body’s most basic functions, like breathing, as well as higher order processing such as thinking and movement. So tumors that develop in a child’s central nervous system, whether the brain or spinal cord, can significantly impact the body’s normal functioning. Exactly what impact stems primary from where the tumor is located, how quickly it grows, and how much damage it causes to the healthy, but extremely delicate, tissues of the spinal cord and brain. Living as a survivor of a spinal cord tumor, whether benign or malignant, usually involves coping with symptoms that stem from (1) the growth of tumor itself and (2) the course of treatment needed to eliminate the tumor.
Taken together, the brain and the spinal cord make up what is known as the “central nervous system” (CNS). The CNS is responsible for our body’s most basic functions, like breathing, as well as higher order processing such as thinking and movement. So tumors that develop in a child’s central nervous system, whether the brain or spinal cord, can significantly impact the body’s normal functioning. Exactly what impact stems primary from where the tumor is located, how quickly it grows, and how much damage it causes to the healthy, but extremely delicate, tissues of the spinal cord and brain. Living as a survivor of a spinal cord tumor, whether benign or malignant, usually involves coping with symptoms that stem from (1) the growth of tumor itself and (2) the course of treatment needed to eliminate the tumor.

 When treatment began, Kyler could not comprehend what was going on, but now one year older, and Kyler can express his feelings about treatment and cope. Ashley said, “Over the last three months, Kyler has really began to cope with the disease. He has began to talk about his feelings and is understanding more and more. We try to explain things to him in a way he can understand.”
When treatment began, Kyler could not comprehend what was going on, but now one year older, and Kyler can express his feelings about treatment and cope. Ashley said, “Over the last three months, Kyler has really began to cope with the disease. He has began to talk about his feelings and is understanding more and more. We try to explain things to him in a way he can understand.”
 On May 3, 2018 Abby was diagnosed with a tumor in her brain. Debbie remembers, “We went into this room that felt like it was smaller than a cardboard box. That is when I heard the words, ‘Your daughter has a tumor in her brain. From where it is, I am thinking it is a cancer that children are known to get.
On May 3, 2018 Abby was diagnosed with a tumor in her brain. Debbie remembers, “We went into this room that felt like it was smaller than a cardboard box. That is when I heard the words, ‘Your daughter has a tumor in her brain. From where it is, I am thinking it is a cancer that children are known to get. 
 Radiation started just after Abby’s 7th birthday. After a few treatments, Abby’s scalp began to become sore so Debbie knew it was time to cut her hair shorter. Later, the radiation would take her hair. The harsh treatments made Abby see flashes of light and smell weird smells. These treatments required her to be face down and strapped to a board, which Abby did not like. Abby was able to ring the bell on July 19th after 30 rounds of radiation. On August 28, 2018, Abby started maintenance chemotherapy which will last until July 2019.
Radiation started just after Abby’s 7th birthday. After a few treatments, Abby’s scalp began to become sore so Debbie knew it was time to cut her hair shorter. Later, the radiation would take her hair. The harsh treatments made Abby see flashes of light and smell weird smells. These treatments required her to be face down and strapped to a board, which Abby did not like. Abby was able to ring the bell on July 19th after 30 rounds of radiation. On August 28, 2018, Abby started maintenance chemotherapy which will last until July 2019.
 Before beginning a discussion of general statistics relating to spinal cord tumors, it is important to note up front several key issues.
Before beginning a discussion of general statistics relating to spinal cord tumors, it is important to note up front several key issues. Meet Taylor, 16-year-old ambitious designer and entrepreneur. Taylor was determined to live life to the fullest, and wanted to be known as “a kid with cancer, never a cancer kid.” She didn’t want cancer to define her. Devastatingly, she passed away after a five year battle with cancer. Sue, her mother, said, “Taylor believed in life that all you need is love, and her memory is indelibly imprinted onto the hearts of everyone she left behind.”
Meet Taylor, 16-year-old ambitious designer and entrepreneur. Taylor was determined to live life to the fullest, and wanted to be known as “a kid with cancer, never a cancer kid.” She didn’t want cancer to define her. Devastatingly, she passed away after a five year battle with cancer. Sue, her mother, said, “Taylor believed in life that all you need is love, and her memory is indelibly imprinted onto the hearts of everyone she left behind.”
 In an excerpt from her book, “Paint Your Hair Blue, A Celebration of Life with Hope for Tomorrow in the Face of Pediatric Cancer” Sue writes: “Taylor’s life was not only about what she accomplished, but also about what she left behind. Her boundless optimism, even at the bleakest moments, and her zest for life, even as death neared, taught me more about love than I thought there was to know. Taylor believed in life that all you need is love, and her memory is indelibly imprinted onto the hearts of everyone she left behind.”
In an excerpt from her book, “Paint Your Hair Blue, A Celebration of Life with Hope for Tomorrow in the Face of Pediatric Cancer” Sue writes: “Taylor’s life was not only about what she accomplished, but also about what she left behind. Her boundless optimism, even at the bleakest moments, and her zest for life, even as death neared, taught me more about love than I thought there was to know. Taylor believed in life that all you need is love, and her memory is indelibly imprinted onto the hearts of everyone she left behind.”

 “It is hard to imagine what I felt. It was as if someone took my breath away and I found myself struggling just to breathe. As parents we don’t have the luxury of falling apart, and I quickly rallied to ask about the x-ray done in September when I was told that my son was constipated. They pulled the x-ray and the mass was in the same place that they misdiagnosed as constipation” remembers Patricia.
“It is hard to imagine what I felt. It was as if someone took my breath away and I found myself struggling just to breathe. As parents we don’t have the luxury of falling apart, and I quickly rallied to ask about the x-ray done in September when I was told that my son was constipated. They pulled the x-ray and the mass was in the same place that they misdiagnosed as constipation” remembers Patricia.