

About Childhood Non-Hodgkin Lymphoma (NHL)
 Non-Hodgkin Lymphoma (NHL) is a specific type of cancer that begins in the body’s immune system, in cells known as lymphocytes. While there are a variety of different classifications of NHL—usually based on key features such as the size, shape, and growth pattern of the cancerous cells—most children are diagnosed with one of three distinct types of NHL (the other types are mainly diagnosed in adults). While all three types of childhood NHL are considered “high grade” (growing aggressively) and diffuse, they are all treated somewhat differently.
Non-Hodgkin Lymphoma (NHL) is a specific type of cancer that begins in the body’s immune system, in cells known as lymphocytes. While there are a variety of different classifications of NHL—usually based on key features such as the size, shape, and growth pattern of the cancerous cells—most children are diagnosed with one of three distinct types of NHL (the other types are mainly diagnosed in adults). While all three types of childhood NHL are considered “high grade” (growing aggressively) and diffuse, they are all treated somewhat differently.
The three types of Non-Hodgkin Lymphoma in children are:
- Lymphoblastic lymphoma (LBL): LBL begins in very young lymphocytes known as lymphoblasts, similar to acute lymphoblastic leukemia (ALL). In most cases, LBL develops from T cells (precursor T-lymphoblastic lymphomas) in the thymus, but occasionally in the tonsils or lymph nodes. B-cell NHL (precursor B-lymphoblastic lymphomas) can develop in lymph nodes in the chest or neck. LBL is an aggressive, quickly growing cancer that can cause breathing problems.
- Burkitt lymphoma (small, non-cleaved cell lymphoma): Burkitt lymphoma accounts for about 40% of all childhood NHL diagnoses in the United States (primarily in boys between the ages of 5-10). In most cases, Burkitt lymphoma starts in the abdomen. In certain parts of Africa, Burkitt lymphoma accounts for nearly all NHL diagnoses and more than 50% of all childhood cancers, and usually forms in the jaw or face. Burkitt lymphoma is one of the fastest-growing cancers and must be treated quickly and aggressively.
- Large cell lymphomas: Large cell lymphomas grow from more mature T or B cells. While this type of lymphoma can develop almost anywhere, it grows more slowly than other lymphomas and is unlikely to spread into the bone marrow or the brain. It is more common in older children and teens. There are two main subtypes: anaplastic large cell lymphoma (ALCL) and diffuse large B-cell lymphoma (DLBCL).
Detection and Diagnosis of Non-Hodgkin Lymphoma
In most cases, diagnosis of non-Hodgkin lymphoma in children comes when a parent or guardian notices unusual symptoms of illness or concern. Although in most cases, these types of symptoms are caused by any number of common childhood illnesses or infections, if your child’s pediatrician believes that lymphoma or another type of cancer may be present, he or she will recommend that you visit an oncologist or other specialist for further diagnostic testing. In most cases, NHL will be diagnosed and classified with a biopsy, in which some or all of the cancerous cells are surgically removed and examined under a microscope.
Childhood NHL can cause a variety of signs and symptoms of illness, usually stemming from where in the body the cancer is growing. Some of the most common symptoms of NHL include:
- Enlarged lymph nodes (lumps under the skin that can be seen or felt) usually in the neck, underarm, collar bone, or groin. They are generally not painful (unlike enlarged lymph nodes resulting from infection).
- Swollen abdomen caused by a tumor in or near the belly or a build-up of fluid because of a tumor. Other signs that of a lymphoma in the abdomen include feeling full after consuming only a small amount of food, pain, nausea, and/or vomiting.
- Shortness of breath or cough caused by a lymphoma growing in the thymus or lymph nodes in the chest.
- Swelling in the face, neck, arms, and upper chest may be caused by a lymphoma pressing on artery and veins near the heart, such as the superior vena cava. Other symptoms of so-called SVC syndrome include trouble breathing, headaches, dizziness, and loss of consciousness.
In addition, NHL can cause so-called B symptoms, which are generalized symptoms but often indicate the presence of an aggressive and quickly-growing lymphoma. B symptoms include:
- Fever and/or chills
- Unexplained weight loss
- Night sweats
- Fatigue (feeling very tired)
Finally, NHL may create symptoms stemming from too few health blood cells (because the lymphoma has spread to the bone marrow and is forcing out healthy blood cells). These symptoms include severe and/or frequent infections, easy bruising and/or bleeding, and fatigue, pale skin, and anemia.
More about Childhood Non-Hodgkin Lymphoma Cancers:
- About Childhood Non-Hodgkin Lymphoma Cancer – Detection and Diagnosis
- Causes, Risk Factors, and Prevention of Childhood Non-Hodgkin Lymphoma Cancer
- What are the signs and symptoms of Childhood Non-Hodgkin Lymphoma Cancer?
- Non-Hodgkin Lymphoma Cancer Treatment
- Non-Hodgkin Lymphoma Cancer – Stages and Prognosis
- What is the expected life span of Childhood Non-Hodgkin Lymphoma Cancer?
- After Treatment – Living as a Childhood Non-Hodgkin Lymphoma Cancer Survivor
Learn More About the Different Types of Childhood Cancers:
- Childhood Brain Tumor Cancer (Brain Stem Tumors)
- Spinal Cord Tumor Cancer
- Childhood Neuroblastoma Cancers
- Childhood Hodgkin Lymphoma Cancers
- Non-Hodgkin Lymphoma Cancers
- Wilms tumor (Kidney Tumors)
- Rhabdomyosarcoma
- Retinoblastoma
- Bone cancer (including osteosarcoma and Ewing sarcoma)
- Leukemia Cancers: Acute lymphocytic (lymphoblastic) leukemia (ALL) Acute myelogenous leukemia (AML); Juvenile myelomonocytic leukemia (JMML)
- Hepatoblastoma (Liver Cancer)
- Rhabdoid Tumors
Together, we can make a difference.
Donate today because kids can’t fight cancer alone®.

About American Childhood Cancer Organization
The American Childhood Cancer Organization was founded in 1970 by parents of children and adolescents diagnosed with cancer. As the nation’s oldest and largest grassroots organization dedicated to childhood cancer, ACCO is committed to shaping policy, supporting research, raising awareness, and providing free educational resources to kids with cancer, survivors, and their families. Additionally, ACCO is the sole U.S. member of Childhood Cancer International (CCI) and has helped support more than half a million families over the past 50 years. Help make childhood cancer a national health priority because kids can’t fight cancer alone®.
For more information about how ACCO can help your family, call 855.858.2226 or visit:
 The good news is that for most patients, the long-term prognosis for childhood Hodgkin lymphoma is excellent. For patients who have been through months or even years of difficult chemotherapy and radiation therapy, it is easy to see the final treatment—the declaration of “cancer free” or even “cured”—as the final destination of a long journey. Survivorship, however, is in fact its own journey, and one that can also be extremely challenging, both physically and emotionally.
The good news is that for most patients, the long-term prognosis for childhood Hodgkin lymphoma is excellent. For patients who have been through months or even years of difficult chemotherapy and radiation therapy, it is easy to see the final treatment—the declaration of “cancer free” or even “cured”—as the final destination of a long journey. Survivorship, however, is in fact its own journey, and one that can also be extremely challenging, both physically and emotionally. Hodgkin lymphoma is a specific type of cancer that starts within white blood cells called lymphocytes found in the lymph (or lymphatic) system. Hodgkin lymphoma (HL) can be diagnosed in individuals of all ages, but is most prevalent in adolescents between the ages of 15-19 and again in adults older than 55. It is rare in children under the age of five. When classified as a type of childhood cancer, HL accounts for about 6% of all childhood cancers; however, most statistics relating to HL do not distinguish between diagnoses in children, adolescents, and adults.
Hodgkin lymphoma is a specific type of cancer that starts within white blood cells called lymphocytes found in the lymph (or lymphatic) system. Hodgkin lymphoma (HL) can be diagnosed in individuals of all ages, but is most prevalent in adolescents between the ages of 15-19 and again in adults older than 55. It is rare in children under the age of five. When classified as a type of childhood cancer, HL accounts for about 6% of all childhood cancers; however, most statistics relating to HL do not distinguish between diagnoses in children, adolescents, and adults. When a child is diagnosed with most types of childhood cancer, including neuroblastoma, a critical part of the diagnosis is the “stage” of the disease. The stage of the disease indicates how far the disease has spread or progressed from the site of the original tumor. In the case of neuroblastoma, there are currently two methodologies in use to determine staging.
When a child is diagnosed with most types of childhood cancer, including neuroblastoma, a critical part of the diagnosis is the “stage” of the disease. The stage of the disease indicates how far the disease has spread or progressed from the site of the original tumor. In the case of neuroblastoma, there are currently two methodologies in use to determine staging. Neuroblastoma is a form of childhood cancer that begins in the early development of nerve cells. Because this rare form of cancer usually begins when the sympathetic nervous system is developing in an embryo or fetus, it occurs most often in infants and very young children, and is extremely rare in children over the age of 10. And because it begins when nerve cells are developing very quickly, the cancer’s development within each child can vary widely: some neuroblastomas grow and spread very quickly while other neuroblastomas grow very slowly. In some cases, the cancerous cells simply disappear on their own, while in other cases, the cancerous cells mature into normal nerve cells. Therefore, treatment for neuroblastoma often depends, upon other factors, on the stage and risk grouping of the cancer, as well as on the age of the child.
Neuroblastoma is a form of childhood cancer that begins in the early development of nerve cells. Because this rare form of cancer usually begins when the sympathetic nervous system is developing in an embryo or fetus, it occurs most often in infants and very young children, and is extremely rare in children over the age of 10. And because it begins when nerve cells are developing very quickly, the cancer’s development within each child can vary widely: some neuroblastomas grow and spread very quickly while other neuroblastomas grow very slowly. In some cases, the cancerous cells simply disappear on their own, while in other cases, the cancerous cells mature into normal nerve cells. Therefore, treatment for neuroblastoma often depends, upon other factors, on the stage and risk grouping of the cancer, as well as on the age of the child. The central nervous system (CNS) is composed of the brain and the spinal cord, a delicate and sensitive column of nerves protected by the boney vertebrae of the spine. Statistically, CNS cancers are all grouped together as “brain and spinal cord tumors”, but of course in reality, there are a number of different and distinct types of spinal cord tumors, and each specific tumor requires a unique treatment approach and carries its own outlook for long-term survivorship.
The central nervous system (CNS) is composed of the brain and the spinal cord, a delicate and sensitive column of nerves protected by the boney vertebrae of the spine. Statistically, CNS cancers are all grouped together as “brain and spinal cord tumors”, but of course in reality, there are a number of different and distinct types of spinal cord tumors, and each specific tumor requires a unique treatment approach and carries its own outlook for long-term survivorship.
 surgery. After reading the scans, doctors determined that her intestines and stomach were severely damaged but no holes were present saying that she
surgery. After reading the scans, doctors determined that her intestines and stomach were severely damaged but no holes were present saying that she 

 When classifying childhood cancers and discussing important statistics, tumors of the brain and tumors of the spinal cord are often lumped together as one broad grouping (although, of course, when diagnosing childhood cancer, each tumor is specified as a more specific “type”). And in general, treatment options for both spinal cord tumors and brain tumors are the same, usually consisting of some combination of
When classifying childhood cancers and discussing important statistics, tumors of the brain and tumors of the spinal cord are often lumped together as one broad grouping (although, of course, when diagnosing childhood cancer, each tumor is specified as a more specific “type”). And in general, treatment options for both spinal cord tumors and brain tumors are the same, usually consisting of some combination of Meet Emma…
Meet Emma…
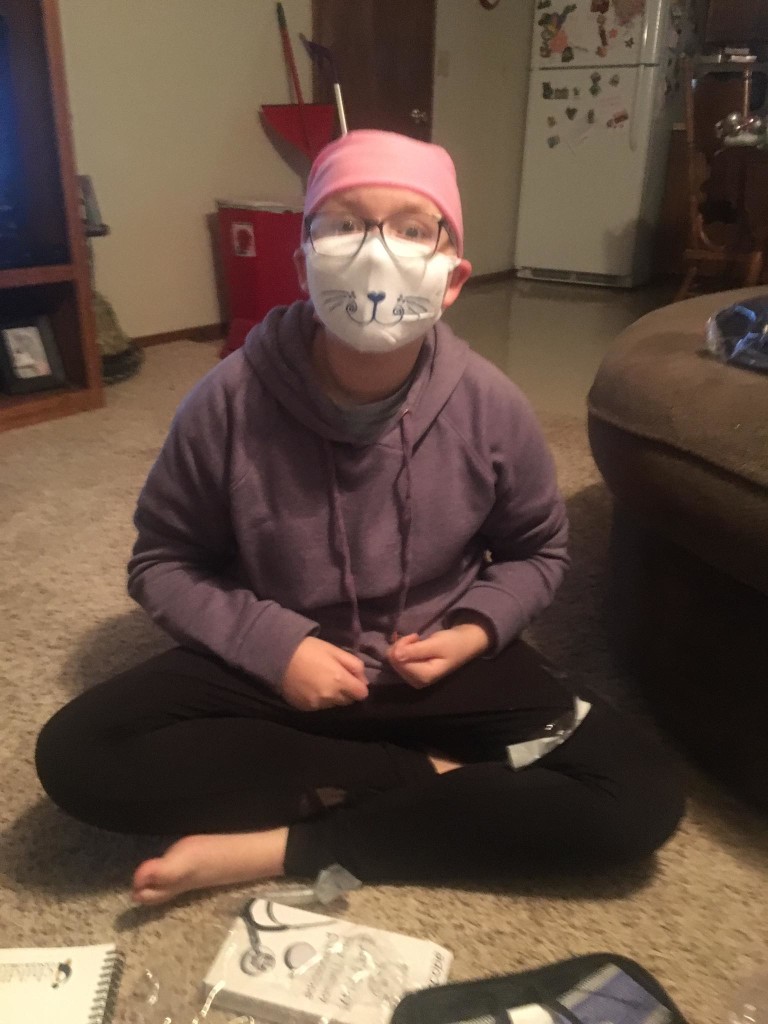
 In the span of ten minutes, Emma’s life changed forever. Megan said that the doctor said, “we see a mass, she is being flown to Oklahoma City.” It took a few minutes before I could catch my breath. I held Emma’s hand and I told her straight up. “Emma, the doctors say they see a tumor and we have to fly to Oklahoma City for another doctor to look at you.” Emma said, “Momma, I will be your angel, and when it is time for you to come, I will come get you.” Heartbreaking.
In the span of ten minutes, Emma’s life changed forever. Megan said that the doctor said, “we see a mass, she is being flown to Oklahoma City.” It took a few minutes before I could catch my breath. I held Emma’s hand and I told her straight up. “Emma, the doctors say they see a tumor and we have to fly to Oklahoma City for another doctor to look at you.” Emma said, “Momma, I will be your angel, and when it is time for you to come, I will come get you.” Heartbreaking. an MRI was performed two days later. The next day, the tumor was removed during her craniotomy. After a preliminary diagnosis of medulloblastoma that was believed to be cancerous, it was confirmed two days later. Treatment has consisted of a port placement, 30 proton therapy treatments, lumbar puncture, chemotherapy, MRI’s of the spine and head under general anesthesia, bone targeted therapies (BTT), bilateral tubes, and multiple hospitalizations. Since Emma’s tumor is so rare, she is currently in a trial where she gets 25% less chemo and proton therapy doses. She’s the only one participating in this study because of the rarity of the tumor. Her results will help to change the way cancer is treated.
an MRI was performed two days later. The next day, the tumor was removed during her craniotomy. After a preliminary diagnosis of medulloblastoma that was believed to be cancerous, it was confirmed two days later. Treatment has consisted of a port placement, 30 proton therapy treatments, lumbar puncture, chemotherapy, MRI’s of the spine and head under general anesthesia, bone targeted therapies (BTT), bilateral tubes, and multiple hospitalizations. Since Emma’s tumor is so rare, she is currently in a trial where she gets 25% less chemo and proton therapy doses. She’s the only one participating in this study because of the rarity of the tumor. Her results will help to change the way cancer is treated.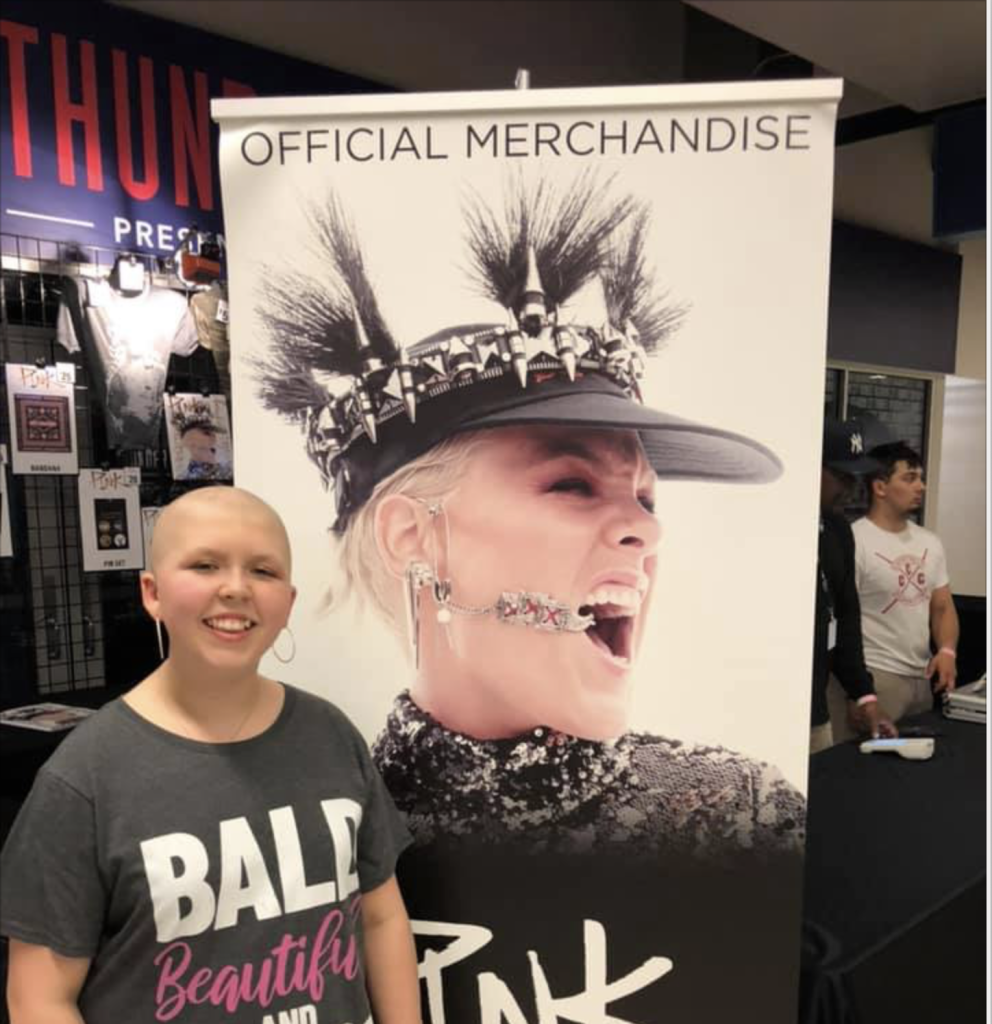 As a result of her diagnosis, Emma suffers from anxiety and depression, decreased fine motor skills and complete left sided deafness. However, Megan says, “She has finally embraced beauty and that it comes in lots of different ways. She is funny and spirited – and yet will lay in my lap and cry often at night.” Emma can be described as ornery, witty and a quick thinker – and her mom wouldn’t have it any other way.
As a result of her diagnosis, Emma suffers from anxiety and depression, decreased fine motor skills and complete left sided deafness. However, Megan says, “She has finally embraced beauty and that it comes in lots of different ways. She is funny and spirited – and yet will lay in my lap and cry often at night.” Emma can be described as ornery, witty and a quick thinker – and her mom wouldn’t have it any other way.