Childhood leukemia is often pointed to as childhood cancer research’s success story. Just 60 years ago, almost no child with leukemia survived more than a few years, but today, thanks to new discoveries and advances in treatment, 90% of children with the most common type of leukemia will survive. That progress is certainly worth celebrating, but these statistics don’t tell the whole story. Let’s take a closer look at what these numbers really mean for children with leukemia. 
What We Mean by “Survival”
When we talk about long-term survival for any childhood cancer, including leukemia, it is important to understand that oncologists and cancer researchers look at the five-year survival rate, or how many children remain cancer-free five years after the end of treatment. In general, children who are still cancer-free after five years are considered “cured” of the disease.
Thanks to advances in treatment methods, the five-year survival rate for childhood leukemia has greatly improved over the past several decades. The five-year survival rate for acute lymphoblastic leukemia (ALL) is now 90%. The five-year survival rate for acute myelogenous leukemia (AML) is lower, at 60-70%. Moreover, the rates can vary greatly depending on subtype and other factors.
These numbers do not, however, provide a specific prognosis for any given child. They are only averages compiled from treated cases of childhood leukemia across the country. Your child’s prognosis and long-term outlook after treatment will be heavily dependent on your child’s diagnosis, response to treatment, and general health.
Prognosis Factors for Childhood Leukemia
Prognosis factors are a series of measurements that your child’s oncology team may use to estimate the degree of risk posed by the cancer and to determine the most promising treatment plan. There are several key prognosis factors that oncologists use when dealing with a leukemia diagnosis. In general, these prognosis factors are the same for ALL and AML, but they do not seem to play as great a role in either guiding treatment or predicting outcomes for AML.
- Risk group: A cancer can be classified as standard risk, high risk, or very high risk. These groupings help determine the intensity of treatment and may impact long-term prognosis.
- Age at diagnosis: For B- cell ALL, children between the ages of 1 and 9 seem to have a more positive prognosis than children under the age of 1 or over the age of 10. Age does not appear to be a prognosis factor in T-cell ALL and AML.
- Initial white blood cell count: Very high white blood cell counts at diagnosis is generally considered high risk or very high risk.
- Subtype: There are many subtypes of leukemia, and some tend to be less aggressive and more responsive to treatment than others. For example, children diagnosed with pre-B, common, or early pre-B-cell ALL seem to have a more positive prognosis than children with mature B-cell leukemia, although B-cell ALL can also have a more positive prognosis if treated with intensive chemotherapy.
- Gender: In general, girls seem to have a slightly better prognosis than boys, though this gap has shrunk in recent years thanks to today’s advanced treatment options.
- Race/ethnicity: African-American and Hispanic children may have a slightly worse prognosis than other ethnicities.
- Spread to other organs: If the leukemia has spread into the fluid around the brain and spinal cord, and the testicles in boys, it is usually classified as high-risk or very high-risk.
- Number of chromosomes and chromosome translocations: Some studies have begun to link longer-term prognosis with the number of chromosomes within the leukemia cells, as well as with translocations between specific chromosomes (when part of a chromosome breaks off and attaches to another).
- Response to treatment: The initial reduction of leukemia cells in the bone marrow during the first one to two weeks of chemotherapy may help determine long-term prognosis. If the leukemia does not respond as expected in this time frame, most oncologists will move to a more intensive treatment protocol.
Life for Childhood Leukemia Survivors
For several years after finishing treatment for leukemia, children will need to have regular exams to check for signs that the cancer has returned, as well as to monitor for side effects of treatment. Some side effects may appear during treatment or soon after the end, while others might not surface until adulthood.
Side effects of childhood leukemia treatment can include:
- Social and emotional challenges
- Developmental delays/learning problems
- Growth delays
- Secondary cancers
- Heart, lung, and bone problems
- Fertility problems
While all childhood leukemia survivors have a greater risk of developing certain health problems as a result of their treatment, most side effects can be managed with proper medical care. It’s important that, even as adults, survivors continue to have regular health checks and are upfront with their healthcare providers about their cancer history.
Kaydence’s Story: Surviving ALL
Kaydence is no ordinary 7-year-old. She’s a talented budding artist with a penchant for donkeys, and she’s a survivor of acute lymphoblastic leukemia. 
There was nothing ordinary about Kaydence’s cancer journey, either. She was found to have two rare chromosome mutations that classified her cancer as very high risk, and when she didn’t respond to the initial treatment, her parents and treatment team decided to move forward with CAR T-cell immunotherapy, a novel treatment that trains the patient’s own immune cells to target and kill the cancer cells.
It wasn’t an easy road. She spent 10 days on life support fighting septic shock two weeks after diagnosis. She went into anaphylactic shock after her T-cell infusion. She had to re-learn how to stand, walk, use her hands and fingers, and go to the toilet. But despite all the setbacks, Kaydence’s treatment was successful. She has been in remission since March 2019. Her immune system is still suppressed, so she has to take extra precautions to make sure she doesn’t get sick, and her doctors continue to monitor her closely for side effects or any signs of her cancer returning. But for her part, Kaydence is enjoying being her 7-year-old self: painting and crafting, playing with her siblings, and just being a normal kid.
September is Leukemia and Lymphoma Awareness Month. Help kids like Kaydence by making a donation to the American Childhood Cancer Organization to honor their fight during Leukemia Awareness Month. Your gift helps provide educational resources and support programs for children with cancer, survivors, and their families, as well as raise awareness about childhood cancer and the need for more research.
Together, we can make a difference.
Donate today… because kids can’t fight cancer alone®.

More about Childhood Leukemia Cancers:
- About Childhood Leukemia Cancer – Detection and Diagnosis
- Causes, Risk Factors, and Prevention of Childhood Leukemia Cancer
- What are the signs and symptoms of Childhood Leukemia Cancer?
- Childhood Leukemia Cancer Treatment
- What is the expected life span of Childhood Leukemia Cancer?
- After Treatment – Living as a Childhood Leukemia Cancer Survivor
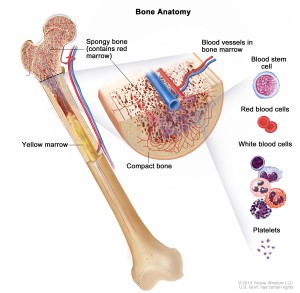 Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow.
Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow. Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL.
Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL. Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy.
Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy. Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally.
Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally. Any discussion of prognosis or outlook is usually based on five-year survival rates, or the percentage of children with a specific type of cancer who live at least five years after their initial diagnosis. These numbers are based on studies performed at least five years ago, and so may not reflect improvement in treatment options for some types of cancers. Moreover, these numbers are merely averages and do not indicate the outlook or prognosis for your specific child. Your child’s oncologist will be able to give you a better understanding of your child’s unique case based on his or her type of cancer, age, general health, and response to treatment.
Any discussion of prognosis or outlook is usually based on five-year survival rates, or the percentage of children with a specific type of cancer who live at least five years after their initial diagnosis. These numbers are based on studies performed at least five years ago, and so may not reflect improvement in treatment options for some types of cancers. Moreover, these numbers are merely averages and do not indicate the outlook or prognosis for your specific child. Your child’s oncologist will be able to give you a better understanding of your child’s unique case based on his or her type of cancer, age, general health, and response to treatment.

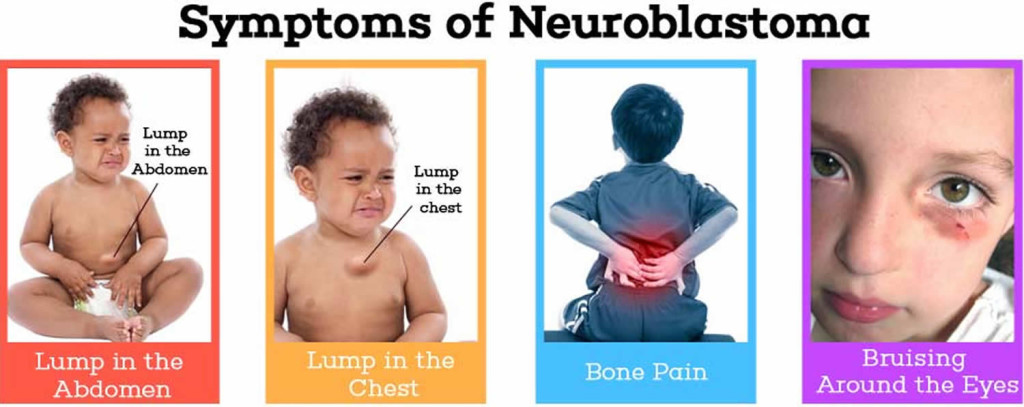 In many cases, symptoms of neuroblastoma are caused by a tumor, or mass of cancerous cells, that becomes visible through the skin or begins to press on other organs of the body. The location of the primary tumor will impact the specific symptoms the child is experiencing. For instance:
In many cases, symptoms of neuroblastoma are caused by a tumor, or mass of cancerous cells, that becomes visible through the skin or begins to press on other organs of the body. The location of the primary tumor will impact the specific symptoms the child is experiencing. For instance: