 THE ACCESS TO CHILDHOOD CANCER ESSENTIALS (ACCESS) INITIATIVE ANNOUNCES TRANSFORMATIVE PROGRAMS TO INCREASE ACCESS TO CRITICAL MEDICINES
THE ACCESS TO CHILDHOOD CANCER ESSENTIALS (ACCESS) INITIATIVE ANNOUNCES TRANSFORMATIVE PROGRAMS TO INCREASE ACCESS TO CRITICAL MEDICINES
• Multistakeholder partnership seeks to enhance care for children with cancer in Africa
• Provides life-saving cancer medicines to children in Ethiopia in collaboration with Teva
• Funds critical research on childhood cancer medicine needs and access barriers in East Africa
FOR IMMEDIATE RELEASE – January 13, 2019 – Washington, D.C. Access to Childhood Cancer Essentials (ACCESS) today announced two initiatives with partners across sectors to improve the lives of children with cancer in Africa. The first, in collaboration with Teva Pharmaceutical Industries Ltd. provides essential, life-saving cancer medicines to children in Ethiopia, and the second funds critical research on childhood cancer medicine needs and access barriers in East Africa with the aim of improving future procurement.
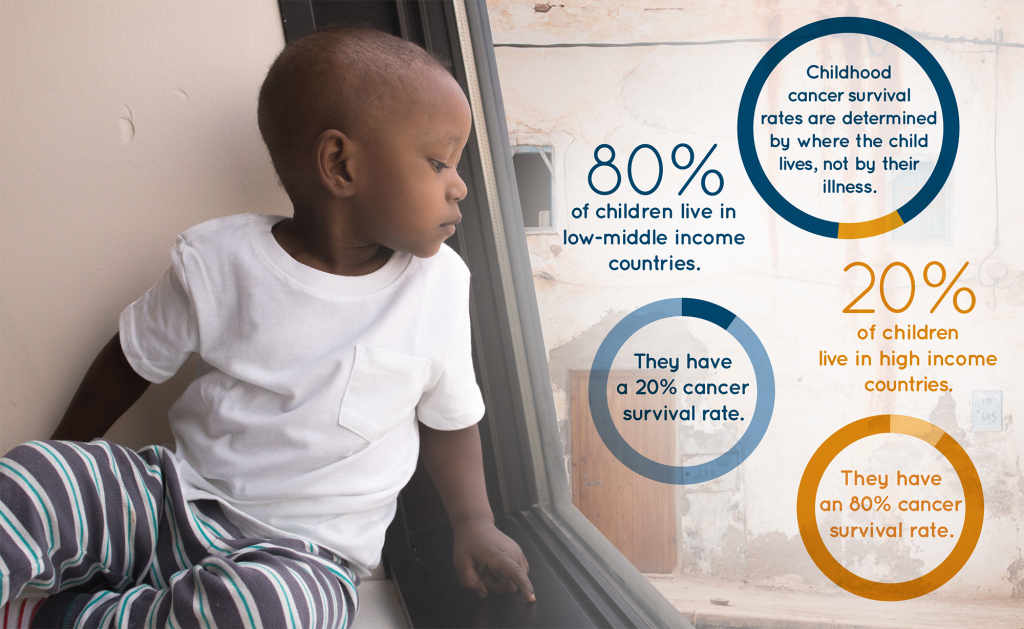
Cancer is the highest non-communicable disease-related cause of death among children globally. While in high-income countries, more than 80 percent of children with cancer are cured, the same percentage of those in low- and middle-income countries die.
“Childhood cancer has no borders; yet, sadly, childhood cancer medicines do,” said Ruth Hoffman, CEO of the American Childhood Cancer Organization, and co-founder of ACCESS. “A major barrier to treating and curing children with cancer in low- and middle-income countries is lack of access to essential medicines.”
 In partnership with Teva Pharmaceuticals, Direct Relief and the Ethiopian Pharmaceutical Fund Supply Agency, ACCESS is providing an emergency provision of 13 cancer medicines from the World Health Organization’s Essential Medicine List—more than 17,000 vials—to children with cancer in Ethiopia.
In partnership with Teva Pharmaceuticals, Direct Relief and the Ethiopian Pharmaceutical Fund Supply Agency, ACCESS is providing an emergency provision of 13 cancer medicines from the World Health Organization’s Essential Medicine List—more than 17,000 vials—to children with cancer in Ethiopia.
This comes as a response to an urgent plea from parents and medical providers of children with cancer, as well as health system leaders. Bitew Tesfaye, a farm laborer, father to seven children, including his six-year old daughter diagnosed with Hodgkin Lymphoma who is awaiting treatment in Addis Ababa shared, “We come from far away, hoping for our children to get well. We start treatment and begin to see light, but, when we are told medicine is not available or only available in a private pharmacy, our hope fades. Now, with access to these medicines, we have hope again.”
“Direct Relief is deeply appreciative to Teva and ACCESS for their leadership and initiative in providing critical treatments to underserved patients in Ethiopia and globally,” said Tom Roane, Strategic Initiatives Director at Direct Relief. “Thanks to this collaboration, patients who would otherwise be unable to access cancer therapies will be able to receive the treatments they need to recover.”
ACCESS is also launching an innovative research program to study the many critical barriers to childhood cancer drug access in Kenya, Rwanda, Uganda, Tanzania and Ethiopia.
“A significant limitation to providing critical medicines to children with cancer in Africa is the lack of knowledge about the scope of the problem,” said Dr. Avram Denburg, Pediatric Oncologist and Principal Investigator, Centre for Global Child Health at The Hospital for Sick Children (SickKids), Canada and co-founder of ACCESS. “The ACCESS East Africa Program is forecasting childhood cancer medicine needs in the region. This will help inform national government procurement efforts and generate evidence of specific barriers to childhood cancer medicine access in each of these countries.” This program is made possible through the generous support of Friends of Cancer Patient’s Ameera Fund and in collaboration with the SickKids Centre for Global Child Health, American Childhood Cancer Organization, Clinton Health Access Initiative and World Bank.

Addressing both immediate and long-term needs, these initiatives represent the power and promise of innovative collaborations between non-profit organizations, the pharmaceutical industry, academia and global health institutions to help save lives of thousands of children with cancer.
For further information or to support these important initiatives, please visit www.accessentials.org.
About Access to Childhood Cancer Essentials
The Access to Childhood Cancer Essentials (ACCESS) Initiative is a multi-stakeholder collaboration focused on improving access to essential medicines for children with cancer globally. Its vision is of a world where the cure of childhood cancer is bounded by the limits of our knowledge, not the limits of our reach. Its mission is to create and implement innovative solutions to childhood cancer drug and radiotherapy access in low and middle income countries so that all children in the world, regardless of where they live, have access to hope for a cure. Visit www.accessentials.org
About Teva
Teva Pharmaceutical Industries Ltd. (NYSE and TASE: TEVA) is a global leader in generic medicines, with innovative treatments in select areas, including CNS, pain and respiratory. We deliver high-quality generic products and medicines in nearly every therapeutic area to address unmet patient needs. We have an established presence in generics, specialty, OTC and API, building on more than a century-old legacy, with a fully integrated R&D function, strong operational base and global infrastructure and scale. We strive to act in a socially and environmentally responsible way. Headquartered in Israel, with production and research facilities around the globe, we employ 45,000 professionals, committed to improving the lives of millions of patients. Learn more at www.tevapharm.com.
About American Childhood Cancer Organization
 The American Childhood Cancer Organization was founded in Washington, D.C. in 1970 by parents of children diagnosed with cancer to advocate for their needs and support research. The nation’s largest grassroots organization at the forefront of the crucial battle against childhood cancer and sole U.S. member of Childhood Cancer International, the ACCO is dedicated to shaping policy, supporting research, raising awareness, and providing educational resources and innovative programs to children with cancer, survivors, and their families. Since its inception, the ACCO has helped support more than half a million families affected by childhood cancer in the U.S. and expended to provide grant funding to support childhood cancer programs in Ethiopia. Visit www.acco.org.
The American Childhood Cancer Organization was founded in Washington, D.C. in 1970 by parents of children diagnosed with cancer to advocate for their needs and support research. The nation’s largest grassroots organization at the forefront of the crucial battle against childhood cancer and sole U.S. member of Childhood Cancer International, the ACCO is dedicated to shaping policy, supporting research, raising awareness, and providing educational resources and innovative programs to children with cancer, survivors, and their families. Since its inception, the ACCO has helped support more than half a million families affected by childhood cancer in the U.S. and expended to provide grant funding to support childhood cancer programs in Ethiopia. Visit www.acco.org.
About Centre for Global Child Health
 The Centre for Global Child Health is the dedicated hub for global child health-focused activities at The Hospital for Sick Children (SickKids). With a rich history of innovation in global paediatric health and a reputable network of global partners, the Centre for Global Child Health is well poised to effectively address global child health issues. The Centre supports the global health agenda through collaborative research grounded in scholarship, sustainable capacity building through education, advocacy for improved maternal and child health and the active communication of results to local, national and inter-national stakeholders. For more information, please visit www.sickkids.ca/globalchildhealth and follow on Twitter @SickKidsGlobal.
The Centre for Global Child Health is the dedicated hub for global child health-focused activities at The Hospital for Sick Children (SickKids). With a rich history of innovation in global paediatric health and a reputable network of global partners, the Centre for Global Child Health is well poised to effectively address global child health issues. The Centre supports the global health agenda through collaborative research grounded in scholarship, sustainable capacity building through education, advocacy for improved maternal and child health and the active communication of results to local, national and inter-national stakeholders. For more information, please visit www.sickkids.ca/globalchildhealth and follow on Twitter @SickKidsGlobal.
About Direct Relief
 Direct Relief is a humanitarian aid organization, active in all 50 states and more than 90 countries worldwide, with a mission to improve the health and lives of people affected by poverty or emergencies. Direct Relief works to equip healthcare providers who care for vulnerable people on an ongoing basis and during emergencies. To achieve this goal, Direct Relief partners with local health providers, leading healthcare companies, and business leaders, to deliver medicines, medical supplies and equipment through transparent, reliable, and cost-effective channels. Direct Relief seeks to support existing health providers over the long term, delivering aid without regard to race, ethnicity, political or religious affiliations, or ability to pay.
Direct Relief is a humanitarian aid organization, active in all 50 states and more than 90 countries worldwide, with a mission to improve the health and lives of people affected by poverty or emergencies. Direct Relief works to equip healthcare providers who care for vulnerable people on an ongoing basis and during emergencies. To achieve this goal, Direct Relief partners with local health providers, leading healthcare companies, and business leaders, to deliver medicines, medical supplies and equipment through transparent, reliable, and cost-effective channels. Direct Relief seeks to support existing health providers over the long term, delivering aid without regard to race, ethnicity, political or religious affiliations, or ability to pay.
Direct Relief partners with leading cancer treatment manufacturers to provide access to life-saving cancer treatment drugs to more than 50 public cancer hospitals around the world. Direct Relief is a member of the globally prominent Union for International Cancer Control (UICC), as well as the specialized cervical cancer association Global Coalition Against Cervical Cancer. In addition, Direct Relief is an Implementing Partner in the UICC’s City Cancer Challenge (C/Can 2025) initiative. More information on Direct Relief’s work on expanding access to cancer treatment can be found at: www.directrelief.org/issue/cancer.
FOR MORE INFORMATION OR TO SET UP AN INTERVIEW
• Dr. Avram Denburg, Staff Oncologist, The Hospital for Sick Children, Toronto, Canada: email Hillete Warner at hillete.warner@sickkids.ca
• Ruth Hoffman, Chief Executive Officer, American Childhood Cancer Organization: email rhoffman@acco.org 202-262-9949


 Meet Olivia, a dynamic and determined 13-year old who loves theater and softball. Olivia is a brave cancer warrior currently fighting acute lymphoblastic t-cell leukemia (ALL).
Meet Olivia, a dynamic and determined 13-year old who loves theater and softball. Olivia is a brave cancer warrior currently fighting acute lymphoblastic t-cell leukemia (ALL).
 Currently, Olivia is in the maintenance phase of treatment with home chemo pills, a monthly clinic chemo, and quarterly lumbar punctures with methotrexate.
Currently, Olivia is in the maintenance phase of treatment with home chemo pills, a monthly clinic chemo, and quarterly lumbar punctures with methotrexate.

 Together, the brain and the spinal cord—the sensitive column of nerve cells inside the vertebrae of the spine—make up our central nervous system (CNS). Cancers of the central nervous system, more commonly called brain and spinal cord tumors, are the second-most common form of cancer in children, after leukemia. Statistically, brain tumors and spinal cord tumors are often grouped together; however in reality, there are a number of different types of tumors of the brain and the spinal cord, each of which requires a unique treatment approach and carries its own prognosis (outlook).
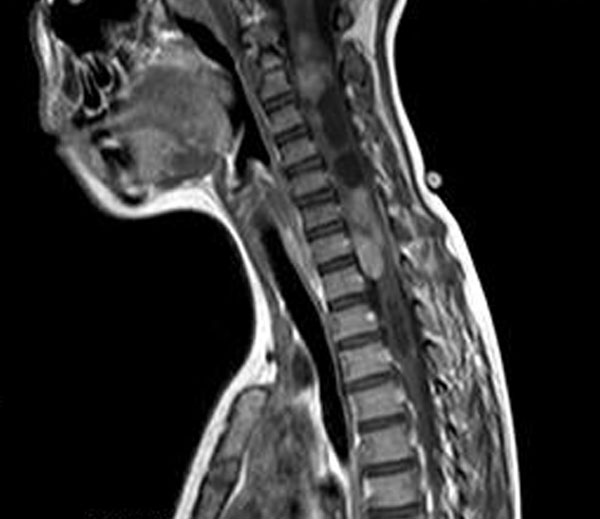
Together, the brain and the spinal cord—the sensitive column of nerve cells inside the vertebrae of the spine—make up our central nervous system (CNS). Cancers of the central nervous system, more commonly called brain and spinal cord tumors, are the second-most common form of cancer in children, after leukemia. Statistically, brain tumors and spinal cord tumors are often grouped together; however in reality, there are a number of different types of tumors of the brain and the spinal cord, each of which requires a unique treatment approach and carries its own prognosis (outlook). When we think of the spine, or backbone, we generally think of it as the part of the skeleton that enables us to stand upright and walk. However, the bones that hold us upright have a second, and potentially even more important, responsibility: protecting a delicate column of nerve tissues that carry messages between the body and the brain. These messages between body and brain are what enables our body to function normally.
When we think of the spine, or backbone, we generally think of it as the part of the skeleton that enables us to stand upright and walk. However, the bones that hold us upright have a second, and potentially even more important, responsibility: protecting a delicate column of nerve tissues that carry messages between the body and the brain. These messages between body and brain are what enables our body to function normally. Meet courageous Colton Whisler, a four-year-old warrior currently battling Perimeningeal Rhabdomyosarcoma, otherwise known as RMS. We were pleased to connect with Colton’s family through The Mark White Show,
Meet courageous Colton Whisler, a four-year-old warrior currently battling Perimeningeal Rhabdomyosarcoma, otherwise known as RMS. We were pleased to connect with Colton’s family through The Mark White Show, 









 The brain and the spinal cord make up what is known as the Central Nervous System (CNS) and together, they control nearly all of our body’s normal functions. The brain is composed of three major parts.
The brain and the spinal cord make up what is known as the Central Nervous System (CNS) and together, they control nearly all of our body’s normal functions. The brain is composed of three major parts.
 Baseball season started in March of 2018 and Damon came home one day after practice saying that his right knee felt like his left one previously. They didn’t really think anything of it – so Damon finished out the baseball season the best he could. Damon’s mother, Tiffiney said, “for a minute the world stopped and went dark. It was Damon’s 16th birthday. It was something that we were somewhat prepared for thanks in part to our spor
Baseball season started in March of 2018 and Damon came home one day after practice saying that his right knee felt like his left one previously. They didn’t really think anything of it – so Damon finished out the baseball season the best he could. Damon’s mother, Tiffiney said, “for a minute the world stopped and went dark. It was Damon’s 16th birthday. It was something that we were somewhat prepared for thanks in part to our spor


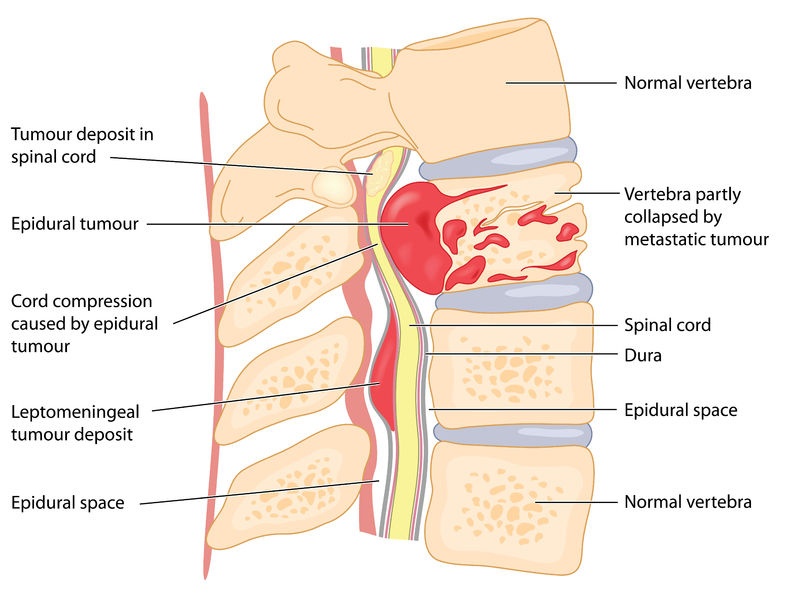
 The central nervous system—including the brain and the spinal cord—grows and develops very quickly during childhood. This rapid rate of growth and development can make treating a brain and/or spinal cord tumor in children especially complicated for several reasons. First, the growth of the tumor can more easily damage the rapidly-changing tissues of the central nervous system (CNS). Second, the tissues of the CNS are extremely sensitive to the potentially damaging impact of chemotherapy, radiation, and other tools required to eliminate the tumor. These two issues are especially concerning when discussing survivorship issues for childhood brain and spinal cord tumors, and may have repercussions well into adulthood.
The central nervous system—including the brain and the spinal cord—grows and develops very quickly during childhood. This rapid rate of growth and development can make treating a brain and/or spinal cord tumor in children especially complicated for several reasons. First, the growth of the tumor can more easily damage the rapidly-changing tissues of the central nervous system (CNS). Second, the tissues of the CNS are extremely sensitive to the potentially damaging impact of chemotherapy, radiation, and other tools required to eliminate the tumor. These two issues are especially concerning when discussing survivorship issues for childhood brain and spinal cord tumors, and may have repercussions well into adulthood.
 By August, Kirby was completely paralyzed from the waist down. The doctors wouldn’t listen. Kirby’s parents decided to take matters into their own hands and took Kirby to a larger hospital to go through more tests. After a tearful meeting with one doctor expressing she didn’t know what was wrong with Kirby, they ordered an MRI. Moments after the MRI was read, the doctor told Sonnie, “we found out what is wrong with your son, he has tumors on his spine and they are spreading. It’s cancer. We need to get him on an airplane on our way to Children’s Hospital.” By noon, the family was on an airplane to Children’s Hospital of Colorado – a home to the Sargent family for the next six months.
By August, Kirby was completely paralyzed from the waist down. The doctors wouldn’t listen. Kirby’s parents decided to take matters into their own hands and took Kirby to a larger hospital to go through more tests. After a tearful meeting with one doctor expressing she didn’t know what was wrong with Kirby, they ordered an MRI. Moments after the MRI was read, the doctor told Sonnie, “we found out what is wrong with your son, he has tumors on his spine and they are spreading. It’s cancer. We need to get him on an airplane on our way to Children’s Hospital.” By noon, the family was on an airplane to Children’s Hospital of Colorado – a home to the Sargent family for the next six months.
