When we hear the word “cancer”, most of us immediately think of adult cancers, the ones at the center of glamorous media campaigns, well-publicized fundraising drives, and focused research efforts, such as breast cancer, colon cancer, prostate cancer, lung cancer, just to name a few. When we hear the words “childhood cancer”, most of us probably think of those same cancers, just in miniature, and assume they have the same causes and the same treatment protocols. In fact, childhood cancers are very, very different than adult cancers, and require very different, specialized treatments.
“Childhood cancer” is a general term describing more than 12 different types of cancer, each of which has numerous sub-types, and each of which requires precise treatment protocols tailored to the small, still-developing bodies of children. The American Childhood Cancer Organization is dedicated to raising awareness about the unique challenges presented by childhood cancer, and the desperate need for new and better treatment protocols that will target these dangerous cancers without the permanent and disabling late term effects that are the all-too-common result of treating childhood cancers with drugs developed to cure adult cancers. We encourage you to read about these most common forms of childhood cancer below, and support the ACCO in its mission to improve the lives of children facing this dreaded disease.
Childhood Leukemia
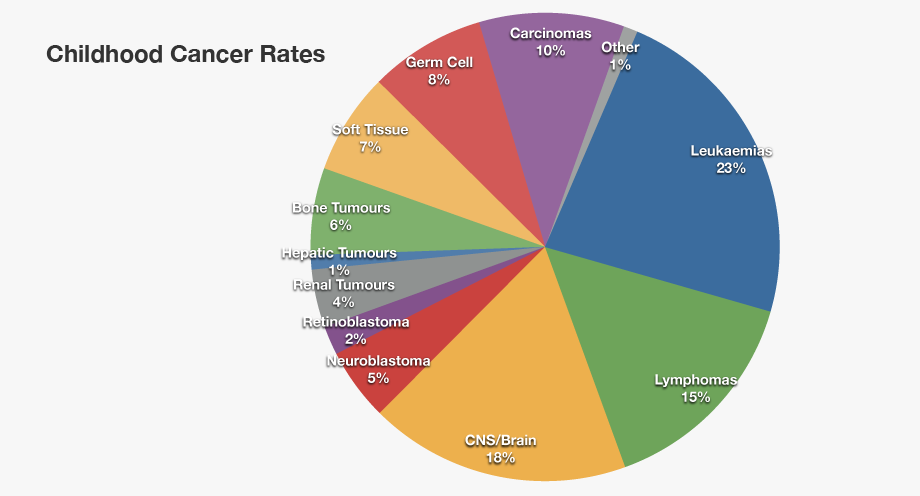
Leukemia is the most common form of childhood cancer, covering more than 30% of all childhood cancers. Leukemia originates in the soft inner part of the bone—the marrow—which is responsible for the development of blood cells. It usually affects the development of white blood cells that are responsible for fighting infection, compromising the body’s ability to fend off disease and heal itself, but leukemia can develop in other types of blood cells as well. The two most common forms of leukemia in children are Acute Lymphocytic Leukemia (ALL) and Acute Myelogenous Leukemia (AML). The good news is that treatments for childhood leukemia have greatly improved in the past decade, and the five-year survival rate is now over 85% for ALL, and over 70% for AML.
Central nervous system and brain tumors
This is the second most widely seen cancer in kids, making up approximately 26% of all childhood cancers. There are several categories of brain tumors and the treatment and prognosis of each of the type is different, depending on a variety of factors including where the tumor is located, the areas of the brain and/or nervous system it is affecting, and how quickly it is growing. It has been observed that children who suffer from such cancer tend to develop tumors in the lower portion of their brain, such as the cerebellum, or the spinal column. Such tumors can cause trouble with object handling, dizziness, blurred vision, vomiting, nausea and headaches.
Neuroblastoma
This type of childhood cancer starts in nerve cells inside a developing fetus or embryo, and grows into tumors in nerve clusters. While neuroblastoma can develop in any part of the body, it is most commonly found in the abdomen. It is by far the most common form of cancer in infants, and is usually diagnosed between the ages of 1 and 2, although can be diagnosed in children as old as 10. Unfortunately, early diagnosis is very difficult, and in 2 out of 3 cases, the disease has already spread to the lymph nodes by the time of diagnosis.
Wilms Tumor
Wilms Tumor develops in or near one or both kidneys, and may even begin developing while the children is still in the womb. It is usually diagnosed in children between the ages of 3 and 4 years old, and is rarely seen in kids above 6 years old. It usually shows as a lump or swelling in the abdomen. The child may often have other symptoms such as poor appetite, nausea, pain, and fever. Wilms Tumor contributes to about 5% of cancers in children.
Bone cancers
Bone cancers in children usually fall into one of two main groups. The most common form—Osteosarcoma—develops in the bones around the knees or near the ends of the long bones of the legs, although it does occasionally occur in the arm bone near the shoulder, the hip bone, or even the jaw. Ewing sarcoma (Ewing family of tumors) is a less common form of bone cancer, usually forming in the pelvis, the chest wall (ribs and shoulder blades), or the middle of the long bones of the leg. While both forms of bone cancer are most commonly diagnosed in teenagers and older children, they can be found in younger children as well. There are some commonalities between these two types of bone cancer, but they respond differently to current treatment protocols.
If you are interested in learning more about these or other forms of childhood cancer, if you would like to know more about the critical need for additional research into the causes and appropriate treatments for childhood cancer, or you would like to support the ACCO’s mission to support all children coping with cancer or its long-term effects and their families, we encourage you to visit www.acco.org to find out how you can help!
For more information about the American Childhood Cancer Organization call 855.858.2226 or visit:






 Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy.
Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy. Any discussion of prognosis or outlook is usually based on five-year survival rates, or the percentage of children with a specific type of cancer who live at least five years after their initial diagnosis. These numbers are based on studies performed at least five years ago, and so may not reflect improvement in treatment options for some types of cancers. Moreover, these numbers are merely averages and do not indicate the outlook or prognosis for your specific child. Your child’s oncologist will be able to give you a better understanding of your child’s unique case based on his or her type of cancer, age, general health, and response to treatment.
Any discussion of prognosis or outlook is usually based on five-year survival rates, or the percentage of children with a specific type of cancer who live at least five years after their initial diagnosis. These numbers are based on studies performed at least five years ago, and so may not reflect improvement in treatment options for some types of cancers. Moreover, these numbers are merely averages and do not indicate the outlook or prognosis for your specific child. Your child’s oncologist will be able to give you a better understanding of your child’s unique case based on his or her type of cancer, age, general health, and response to treatment.
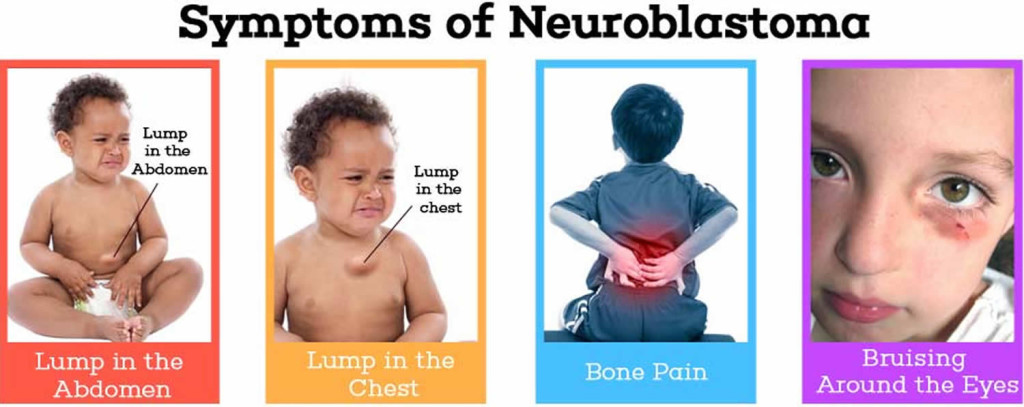 In many cases, symptoms of neuroblastoma are caused by a tumor, or mass of cancerous cells, that becomes visible through the skin or begins to press on other organs of the body. The location of the primary tumor will impact the specific symptoms the child is experiencing. For instance:
In many cases, symptoms of neuroblastoma are caused by a tumor, or mass of cancerous cells, that becomes visible through the skin or begins to press on other organs of the body. The location of the primary tumor will impact the specific symptoms the child is experiencing. For instance: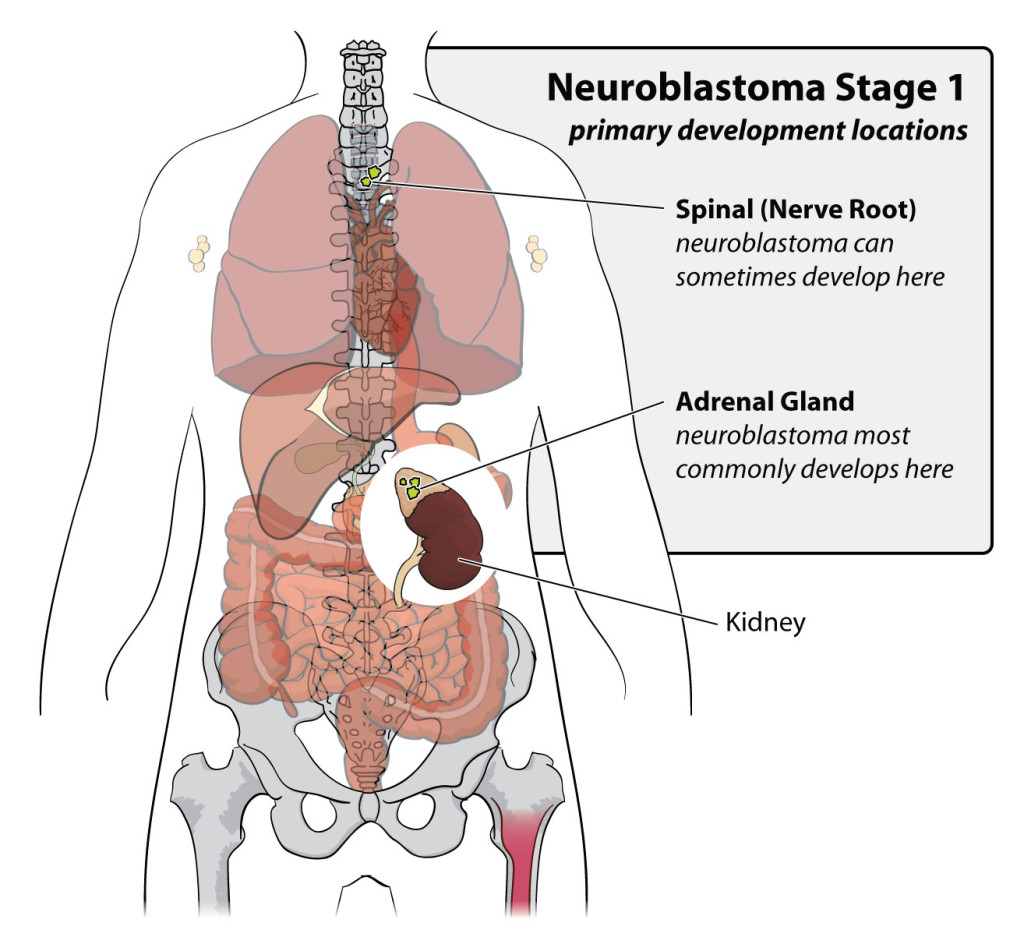 Neuroblastoma is caused by the abnormal development of immature nerve cells known as neuroblasts. As a fetus develops, most neuroblasts grow and eventually become mature nerve cells either before birth or in the first few months after birth. However, in some cases, neuroblasts do not develop correctly. Instead of becoming mature nerve cells, they continue to grow and divide. In some cases, these abnormal neuroblasts simply die off; however, in some rare cases, they develop into tumors or neuroblastoma.
Neuroblastoma is caused by the abnormal development of immature nerve cells known as neuroblasts. As a fetus develops, most neuroblasts grow and eventually become mature nerve cells either before birth or in the first few months after birth. However, in some cases, neuroblasts do not develop correctly. Instead of becoming mature nerve cells, they continue to grow and divide. In some cases, these abnormal neuroblasts simply die off; however, in some rare cases, they develop into tumors or neuroblastoma.
