

Introduction: About Childhood Hodgkin Lymphoma
Childhood Hodgkin lymphoma is a type of cancer that develops in the lymph system, a critical part of the body’s immune system responsible for fighting illness-causing viruses and bacteria. Classical Hodgkin lymphoma is generally characterized by the presence of a particular type of cancer cell known as Reed-Sternberg cells, although a much more rare form of Hodgkin lymphoma known as Nodular lymphocyte-predominant Hodgkin lymphoma is characterized instead by lymphocyte-predominant cells. Childhood Hodgkin lymphoma comprises about 6% of all childhood cancers, and is diagnosed most prevalently in adolescents between the ages of 15-19.
Childhood Hodgkin Lymphoma: Stages
 The “stage” of a disease is a method of determining the extent to which the cancer has grown and spread, and plays a critical role in determining the appropriate course of treatment. Staging childhood Hodgkin lymphoma involves three distinct, yet overlapping, categorizations:
The “stage” of a disease is a method of determining the extent to which the cancer has grown and spread, and plays a critical role in determining the appropriate course of treatment. Staging childhood Hodgkin lymphoma involves three distinct, yet overlapping, categorizations:
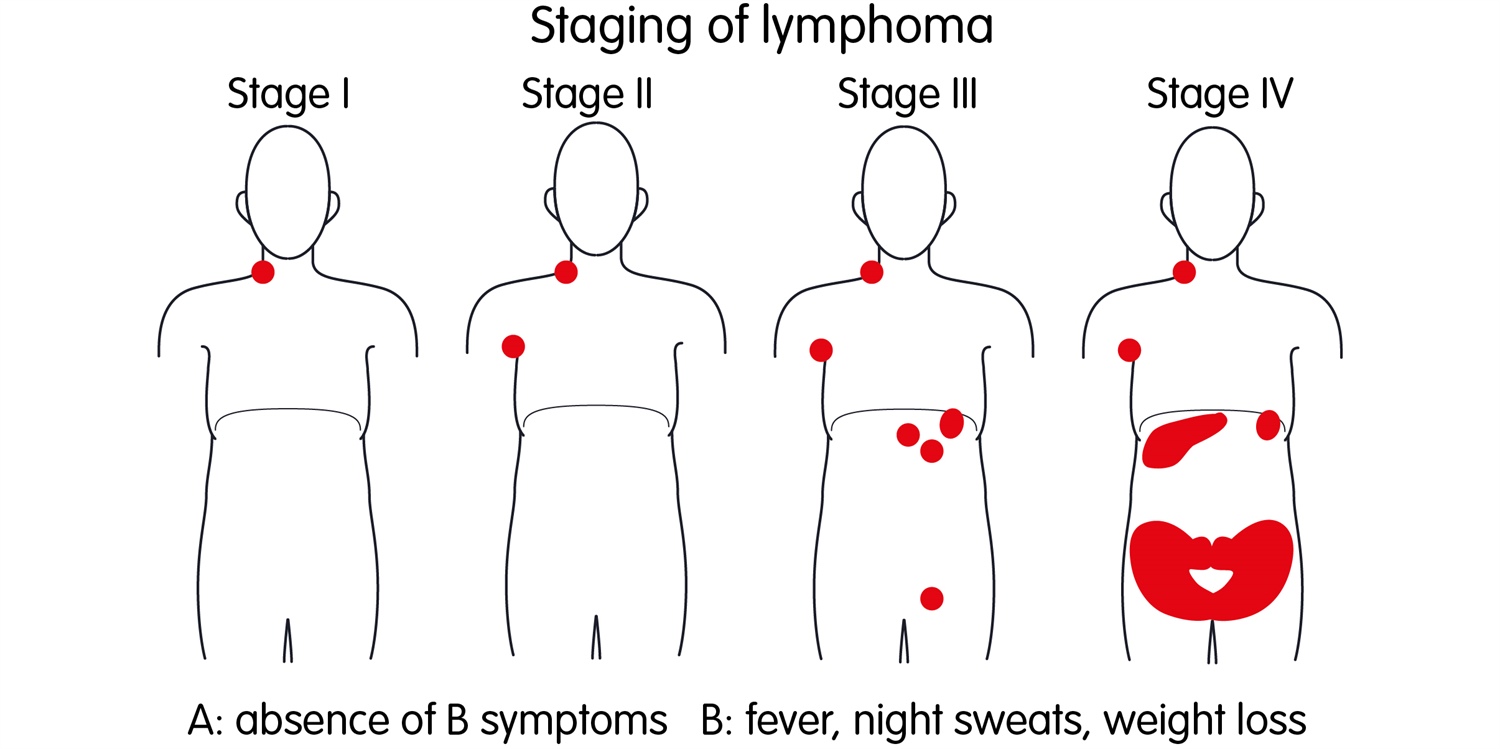
A, B, E, and S: Childhood Hodgkin lymphoma is usually described in one of four distinct ways, preliminary to traditional staging:
- A: Diagnosis with no symptoms
- B: Diagnosis with so-called “B” symptoms: fever, weight loss, and/or night sweats
- E: Cancerous cells have been located in an organ or tissue that may be next to, but is not part of the lymph system
- S: Cancerous cells have been found in the spleen
I, II, III, and IV: Specific stages of childhood Hodgkin lymphoma incorporate the A, B, E, and S descriptions:
- Stage I: Cancerous cells are in one or more lymph nodes, but only one lymph node group. Stage IE involves cancer cells outside the lymph system in one other organ or area of the body.
- Stage II: Cancer cells are found in two or more lymph node groups, either above or below the diaphragm. Stage IIE involves cancer cells in one or more lymph node groups above or below the diaphragm and outside the lymph node groups in an adjacent organ.
- Stage III: Cancerous cells are in one or more lymph node groups above and below the diaphragm. Stage IIIE involves cancer in lymph node groups above and below the diaphragm and outside the lymph system in adjacent organs. Stage IIIS includes cancer cells in lymph node groups above and below the diaphragm and in the spleen, while Stage IIIE+S involves cancer in lymph node groups above and below the diaphragm, in nearby organs, and in the spleen.
- Stage IV: Cancerous cells can be found in the lymph nodes throughout one or more organs, as well as in lymph nodes near those organs, or is in one organ and has spread to lymph nodes far away from that organ, or is in the lung, liver, or bone marrow.
Risk groups: Classical childhood Hodgkin lymphoma is also divided into risk groups depending on the bulk of the tumor(s) (“bulky” tumors are defined as 5 centimeters or larger) and whether the patient has so-called “B” symptoms:
- Low risk: Stage I or Stage II with no bulky tumors or “B” symptoms
- Intermediate risk: Stage I or II with bulky tumors OR “B” symptoms; OR Stage III or IV with no “B” symptoms
- High risk: Stage III or IV with “B” symptoms
Childhood Hodgkin Lymphoma: Outcomes and Prognosis
*Disclaimer: Every case of childhood Hodgkin lymphoma is unique and different. Statistics relating to outcomes and prognosis for Hodgkin lymphoma, such as five-year survival rates, are estimates for informational purposes only. If your child has been diagnosed with childhood Hodgkin lymphoma, his or her oncology team will discuss your child’s prognosis in the specific context of your child’s specific disease and medical history.
In general, childhood Hodgkin lymphoma is considered highly “curable”. This particular form of childhood cancer has been found to be very sensitive to both chemotherapy and radiation therapy, and was, in fact, the first form of cancer to be “cured” with radiation therapy alone or with a combination chemotherapy protocol. As with all childhood cancers, however, the five-year survival rate depends upon the unique nature of each child’s specific disease, the stage of the disease upon diagnosis, and the categorization of risk. For children and adolescents with Stage I or Stage II Hodgkin lymphoma, the overall survival rate is over 90%; however, for children and adolescents with Stage III or Stage IV Hodgkin lymphoma, the overall survival rate may be as low as 70%.
Together, we can make a difference.
Donate today because kids can’t fight cancer alone®.

More about Childhood Hodgkin Lymphoma Cancers:
- About Childhood Hodgkin Lymphoma Cancer – Detection and Diagnosis
- Causes, Risk Factors, and Prevention of Childhood Hodgkin Lymphoma Cancer
- What are the signs and symptoms of Childhood Hodgkin Lymphoma Cancer?
- Childhood Hodgkin Lymphoma Cancer Treatment
- What is the expected life span of Childhood Hodgkin Lymphoma Cancer?
- After Treatment – Living as a Childhood Hodgkin Lymphoma Cancer Survivor
 The Mother’s Day traditions of paper cards and handmade crafts will not be the current reality for all families this year. We know that an inside look into the reality of Mother’s Day may include a family celebrating a child’s successful, but excruciating cancer treatment. We also know that other scenes are filled with moms comforting a sick child in a hospital or even worse, moms shielding a broken heart in the empty silence of a house that, at one time, used to be full of chaos and noise. This unfortunate depiction is often the sad reality left in the devastating wake of childhood cancer.
The Mother’s Day traditions of paper cards and handmade crafts will not be the current reality for all families this year. We know that an inside look into the reality of Mother’s Day may include a family celebrating a child’s successful, but excruciating cancer treatment. We also know that other scenes are filled with moms comforting a sick child in a hospital or even worse, moms shielding a broken heart in the empty silence of a house that, at one time, used to be full of chaos and noise. This unfortunate depiction is often the sad reality left in the devastating wake of childhood cancer.
 Eleven years ago, on May 11, Derek Madsen passed away after a long struggle with an aggressive type of childhood cancer, neuroblastoma, at the age of 11. That year—2006—May 11 was just a few days before Mother’s Day. On that day, Derek’s mother, Cyndie French, was forced to make the most difficult decision a mother can be asked to make: the decision to let her son go, to help Derek take his final breath. So, it seems only appropriate that we begin this special multi-part series on Derek and Cyndie honoring a very brave childhood cancer mother, eleven years after Derek passed away in the loving arms of his family.
Eleven years ago, on May 11, Derek Madsen passed away after a long struggle with an aggressive type of childhood cancer, neuroblastoma, at the age of 11. That year—2006—May 11 was just a few days before Mother’s Day. On that day, Derek’s mother, Cyndie French, was forced to make the most difficult decision a mother can be asked to make: the decision to let her son go, to help Derek take his final breath. So, it seems only appropriate that we begin this special multi-part series on Derek and Cyndie honoring a very brave childhood cancer mother, eleven years after Derek passed away in the loving arms of his family. Cyndie’s goal in sharing her story exclusively with ACCO is to raise awareness about the devastating consequences of a childhood cancer diagnosis on the family. It is easy to discuss the need for greater research into finding a cure for childhood cancer but can be difficult to face the grim realities that families go through—physically, emotionally, and financially—after a cancer diagnosis. Like ACCO, Cyndie’s goal is to shine a light onto those problems, in the hope that bringing this light will also bring a solution: more financial and emotional support for families coping with a cancer diagnosis.
Cyndie’s goal in sharing her story exclusively with ACCO is to raise awareness about the devastating consequences of a childhood cancer diagnosis on the family. It is easy to discuss the need for greater research into finding a cure for childhood cancer but can be difficult to face the grim realities that families go through—physically, emotionally, and financially—after a cancer diagnosis. Like ACCO, Cyndie’s goal is to shine a light onto those problems, in the hope that bringing this light will also bring a solution: more financial and emotional support for families coping with a cancer diagnosis. Over the next several months, ACCO will chronicle Cyndie’s story, from her own perspective. In this multi-part series, we will attempt to offer a comprehensive view into what family life is like during treatment for an aggressive and ultimately terminal case of childhood cancer. Cyndie’s story will include the financial consequences of a cancer diagnosis, the challenge of caring for siblings and maintaining a supportive family structure, the difficulty of helping her child cope with hospital stays and treatment protocols, and the gut-wrenching discussions and decisions that must be faced as treatment fails. In each segment, we will share Cyndie’s goals for helping families cope and share information about ACCO’s mission of support and assistance as well.
Over the next several months, ACCO will chronicle Cyndie’s story, from her own perspective. In this multi-part series, we will attempt to offer a comprehensive view into what family life is like during treatment for an aggressive and ultimately terminal case of childhood cancer. Cyndie’s story will include the financial consequences of a cancer diagnosis, the challenge of caring for siblings and maintaining a supportive family structure, the difficulty of helping her child cope with hospital stays and treatment protocols, and the gut-wrenching discussions and decisions that must be faced as treatment fails. In each segment, we will share Cyndie’s goals for helping families cope and share information about ACCO’s mission of support and assistance as well. Right from the start, Cyndie would like to thank Renée for the dedication, care, and compassion that she has brought to this story. During the year of Derek’s treatment, Renée became more than simply an interested third party, she became a friend. Both Cyndie and Derek came to trust her and welcome her into their lives, even during some of life’s intimate moments. As her photos show, Derek was often angry, frustrated, and scared during his treatment, refusing help from everyone but Cyndie, yet he came to realize that Renée was there to share his story and to honestly and appropriately capture his feelings. ACCO would like to thank Ms. Byers for allowing us to incorporate these amazing photos into our series on Cyndie and Derek.
Right from the start, Cyndie would like to thank Renée for the dedication, care, and compassion that she has brought to this story. During the year of Derek’s treatment, Renée became more than simply an interested third party, she became a friend. Both Cyndie and Derek came to trust her and welcome her into their lives, even during some of life’s intimate moments. As her photos show, Derek was often angry, frustrated, and scared during his treatment, refusing help from everyone but Cyndie, yet he came to realize that Renée was there to share his story and to honestly and appropriately capture his feelings. ACCO would like to thank Ms. Byers for allowing us to incorporate these amazing photos into our series on Cyndie and Derek. Evan Mario Macrone was 11 years old when he was diagnosed with childhood cancer, in August 2015. First, Evan noticed a small lump in his groin while playing with his little brother, Gavin. A biopsy revealed the worst-case scenario: a soft tissue sarcoma. So instead of starting middle school, Evan started an intensive treatment regime involving 17 rounds of chemotherapy, 6 weeks of radiation, and surgery.
Evan Mario Macrone was 11 years old when he was diagnosed with childhood cancer, in August 2015. First, Evan noticed a small lump in his groin while playing with his little brother, Gavin. A biopsy revealed the worst-case scenario: a soft tissue sarcoma. So instead of starting middle school, Evan started an intensive treatment regime involving 17 rounds of chemotherapy, 6 weeks of radiation, and surgery. On March 15, 2017, Evan passed away while traveling to California with the Make a Wish foundation to visit his best friend and see the famous sights of Los Angeles. Unable to make the trip home, Evan was surrounded by his family, including his two beloved brothers Mike and Gavin, and his best friend. He was laid to rest near his family home in Florida.
On March 15, 2017, Evan passed away while traveling to California with the Make a Wish foundation to visit his best friend and see the famous sights of Los Angeles. Unable to make the trip home, Evan was surrounded by his family, including his two beloved brothers Mike and Gavin, and his best friend. He was laid to rest near his family home in Florida. “Evan touched lives in so many ways, more than I could have known. More important, Evan was a kind, gentle, loving, joyful, and giving person. He made sure others in his class understood concepts and went out of his way to assist them and reach out to those he saw may be having difficulty. He gave of himself to his friends and scouts selflessly.
“Evan touched lives in so many ways, more than I could have known. More important, Evan was a kind, gentle, loving, joyful, and giving person. He made sure others in his class understood concepts and went out of his way to assist them and reach out to those he saw may be having difficulty. He gave of himself to his friends and scouts selflessly. Throughout Life I have learned
Throughout Life I have learned Thank you
Thank you Finally, we would like to thank:
Finally, we would like to thank: The goal of the 2017 Childhood Cancer Action Days was to give members of the childhood cancer community, including parents, children with cancer, survivors, healthcare professionals and advocacy groups the opportunity to learn and implement effective advocacy approaches specifically relating to childhood cancer. This two-day event started with a day of formal advocacy training where participants learned critical “tips of the trade” from experienced advocacy experts within the childhood cancer community. On Tuesday, after an inspirational breakfast meeting, participants were off to “The Hill” to meet with their Members of Congress and staff in person to share their stories and show their support for childhood cancer issues currently pending before Congress.
The goal of the 2017 Childhood Cancer Action Days was to give members of the childhood cancer community, including parents, children with cancer, survivors, healthcare professionals and advocacy groups the opportunity to learn and implement effective advocacy approaches specifically relating to childhood cancer. This two-day event started with a day of formal advocacy training where participants learned critical “tips of the trade” from experienced advocacy experts within the childhood cancer community. On Tuesday, after an inspirational breakfast meeting, participants were off to “The Hill” to meet with their Members of Congress and staff in person to share their stories and show their support for childhood cancer issues currently pending before Congress. Advocacy is Ongoing: Keep the Pressure On!
Advocacy is Ongoing: Keep the Pressure On!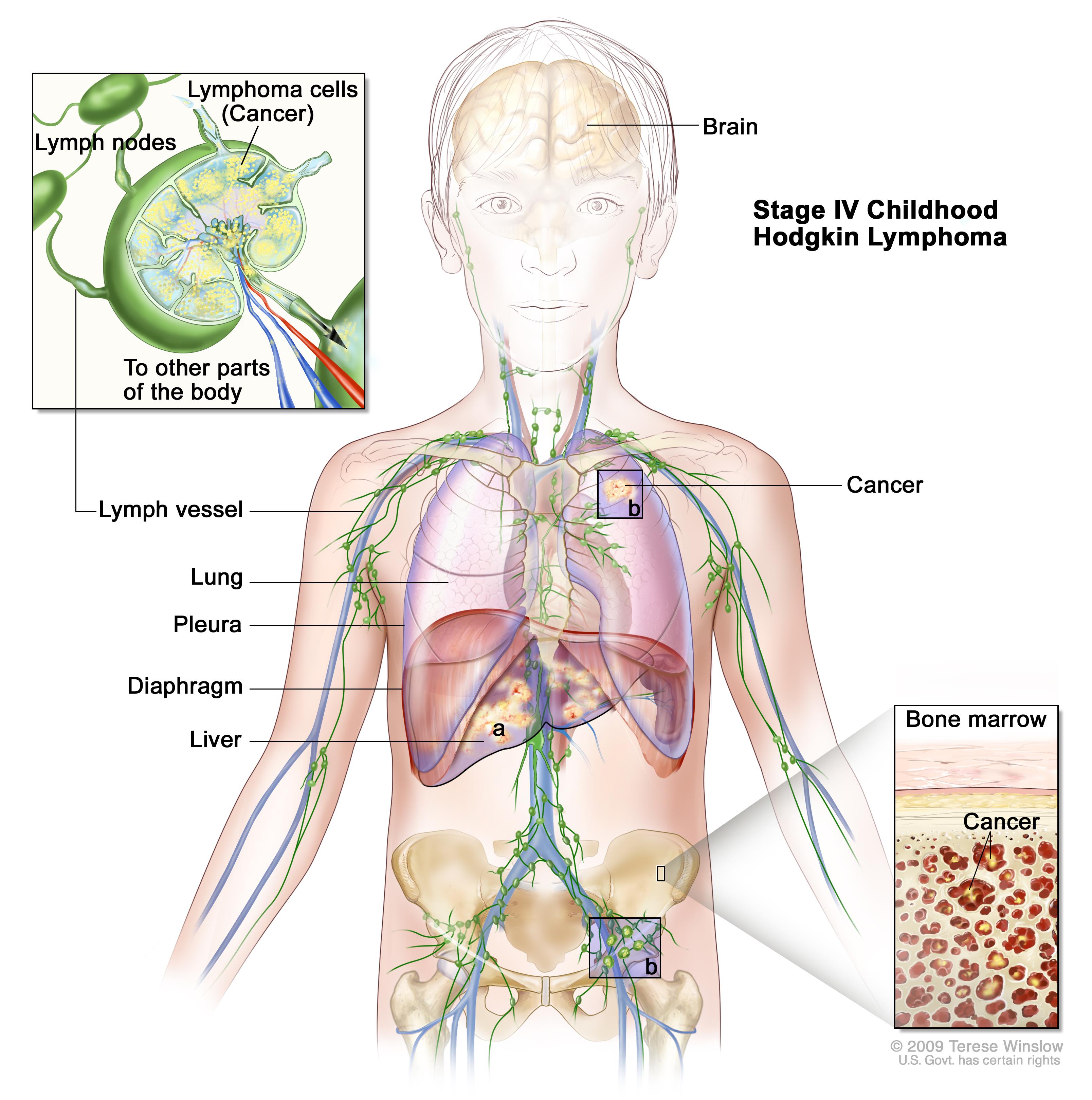


 For the first year of her life, Lexy progressed just like any healthy, happy child, despite the NF1 diagnosis, crawling and starting to take her first shaky steps. But just after her first birthday, her parents noticed that she had stopped trying to walk and had started to drag her left leg as she crawled. Concern turned to alarm when Lexy began clutching her left arm tightly to her chest. A trip to the pediatrician quickly turned into an emergency MRI, the results of which were devastating. A brain tumor the size of a Granny Smith apple was pressing on Lexy’s brain, causing partial paralysis on the left side.
For the first year of her life, Lexy progressed just like any healthy, happy child, despite the NF1 diagnosis, crawling and starting to take her first shaky steps. But just after her first birthday, her parents noticed that she had stopped trying to walk and had started to drag her left leg as she crawled. Concern turned to alarm when Lexy began clutching her left arm tightly to her chest. A trip to the pediatrician quickly turned into an emergency MRI, the results of which were devastating. A brain tumor the size of a Granny Smith apple was pressing on Lexy’s brain, causing partial paralysis on the left side. Most recently, Lexy has been participating in a clinical trial in Pittsburg focused on a vaccine-based approach. The goal of this trial is to convince the body that the tumor is an infection, with the goal of training the body to use its own white blood cells to fight the tumor. Unfortunately, after more than a year in this trial, Lexy’s most recent scans show a tumor that is stable but not shrinking. The unhappy conclusion is that the tumor is likely not going to respond to this form of treatment.
Most recently, Lexy has been participating in a clinical trial in Pittsburg focused on a vaccine-based approach. The goal of this trial is to convince the body that the tumor is an infection, with the goal of training the body to use its own white blood cells to fight the tumor. Unfortunately, after more than a year in this trial, Lexy’s most recent scans show a tumor that is stable but not shrinking. The unhappy conclusion is that the tumor is likely not going to respond to this form of treatment.



 Childhood Hodgkin lymphoma, similarly to adult Hodgkin lymphoma, is a type of malignant cancer of the lymph system, which forms a critical part of the immune system our bodies use to fight disease. Specifically, Hodgkin lymphoma usually begins in lymphocytes, a type of white blood cell responsible for fighting bacteria, viruses, and other foreign invaders. Hodgkin lymphoma makes up about 6% of all childhood cancers. Today, the prognosis for children with Hodgkin lymphoma is significantly higher than even a decade ago, with the five-year survival rate between 90-95%.
Childhood Hodgkin lymphoma, similarly to adult Hodgkin lymphoma, is a type of malignant cancer of the lymph system, which forms a critical part of the immune system our bodies use to fight disease. Specifically, Hodgkin lymphoma usually begins in lymphocytes, a type of white blood cell responsible for fighting bacteria, viruses, and other foreign invaders. Hodgkin lymphoma makes up about 6% of all childhood cancers. Today, the prognosis for children with Hodgkin lymphoma is significantly higher than even a decade ago, with the five-year survival rate between 90-95%.