


 Meet Emma…
Meet Emma…
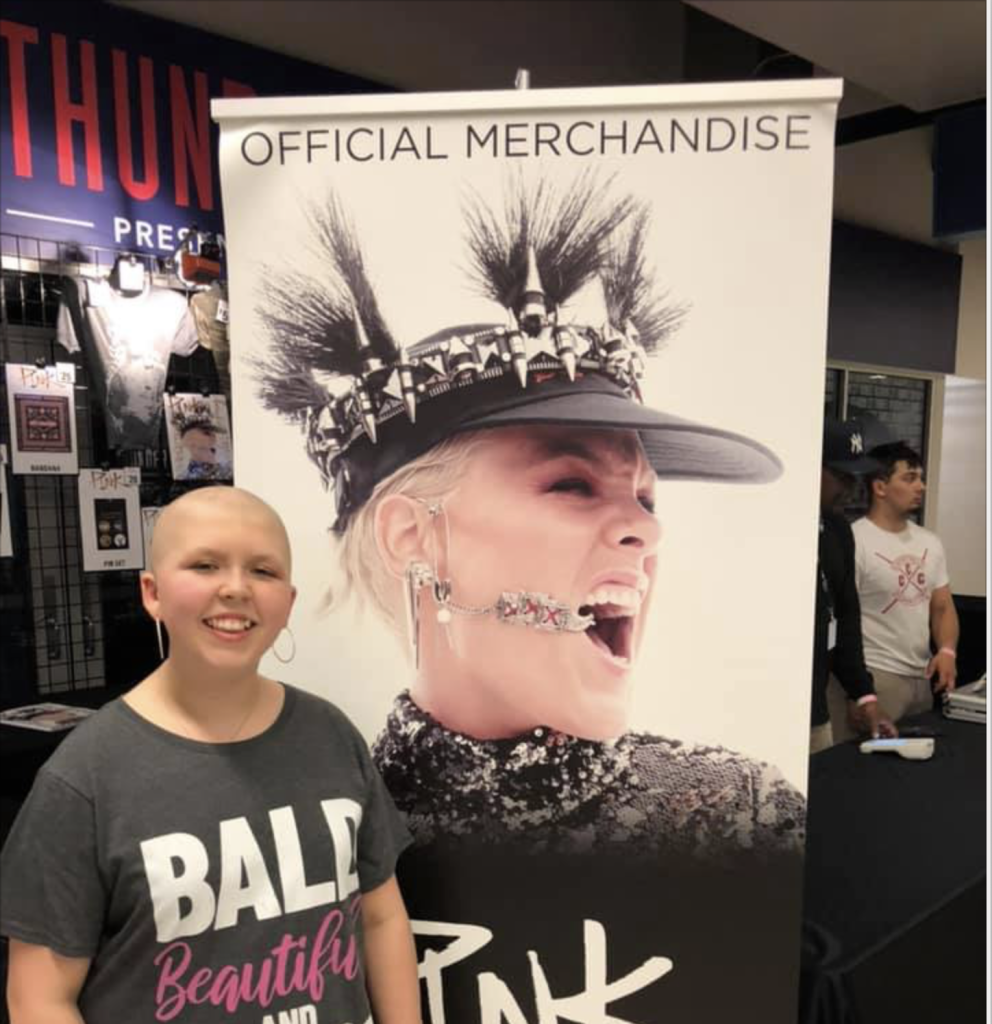
A PBR-loving, supergirl cancer warrior currently fighting stage IV medulloblastoma. She enjoys arts and crafts of all kinds, cooking, playing games and making jewelry. She also loves circuit boards, making slime and loves to paint. She is a huge P!nk fan and was lucky enough to see her live last weekend!
In 2017, Emma was a straight-A student heading into sixth grade. As a 5th grader, she received ‘Student of the Month’ seven times. She was recognized for helping classmates, was on the honor roll, and a member of the student council. She was even a member of the robotics team for a year. Emma’s mother, Megan, said she was called several times throughout the school year because Emma was late for class. It turns out “she took too long hugging her former teachers and other students in the hall and was late,” recalls Megan.
In May 2018, Emma began dropping weight. She started vomiting occasionally but nothing too alarming. She was increasingly lethargic, had no appetite and headaches had started. After one episode of violent vomiting, Megan took Emma to the doctor but without a pattern, the doctor thought it was puberty. After swimming one day, Emma told her mother she was exhausted, which was out of character.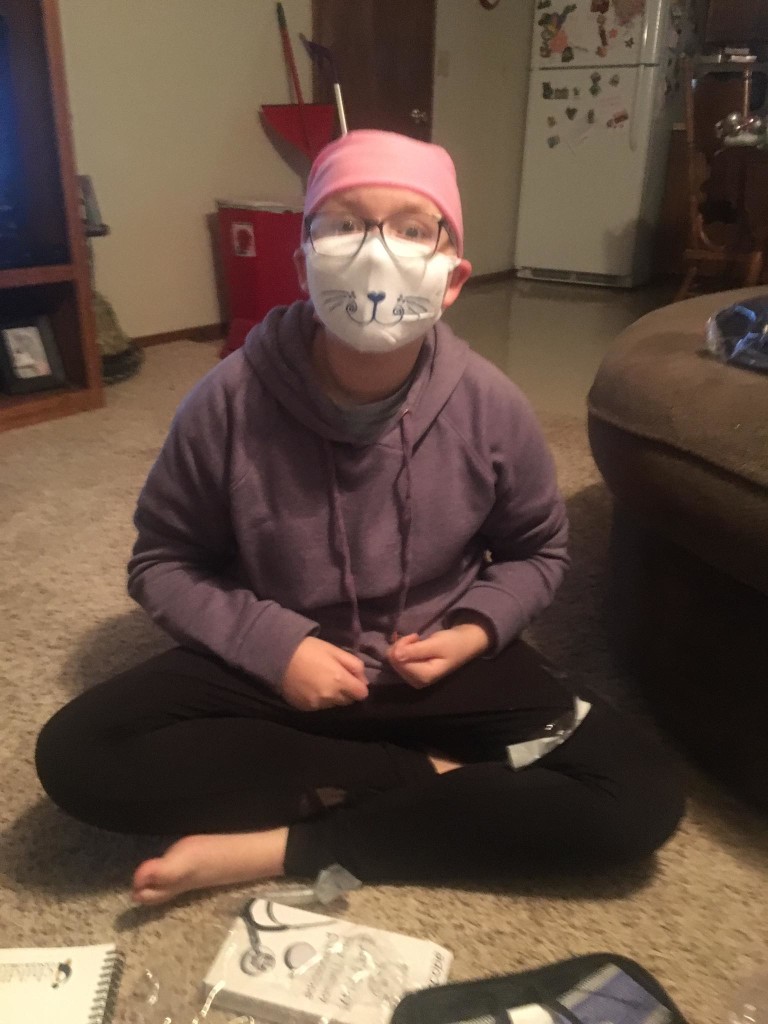
Megan received a call that weekend from Emma’s dad after Emma was found vomiting in her bed. Emma was taken to the emergency room twice in the same day. On the second trip to the ER, a CT was ordered and ten minutes later Emma and her mother were given the news of her Medulloblastoma cancer diagnosis. “We were just in shock. We are still in shock. I have three friends with kids who have brain tumors. Two have died, Emma thought she was dying,” remembers Megan.
 In the span of ten minutes, Emma’s life changed forever. Megan said that the doctor said, “we see a mass, she is being flown to Oklahoma City.” It took a few minutes before I could catch my breath. I held Emma’s hand and I told her straight up. “Emma, the doctors say they see a tumor and we have to fly to Oklahoma City for another doctor to look at you.” Emma said, “Momma, I will be your angel, and when it is time for you to come, I will come get you.” Heartbreaking.
In the span of ten minutes, Emma’s life changed forever. Megan said that the doctor said, “we see a mass, she is being flown to Oklahoma City.” It took a few minutes before I could catch my breath. I held Emma’s hand and I told her straight up. “Emma, the doctors say they see a tumor and we have to fly to Oklahoma City for another doctor to look at you.” Emma said, “Momma, I will be your angel, and when it is time for you to come, I will come get you.” Heartbreaking.
Emma was transferred to OKC and admitted to the PICU where a shunt was placed and an MRI was performed two days later. The next day, the tumor was removed during her craniotomy. After a preliminary diagnosis of medulloblastoma that was believed to be cancerous, it was confirmed two days later. Treatment has consisted of a port placement, 30 proton therapy treatments, lumbar puncture, chemotherapy, MRI’s of the spine and head under general anesthesia, bone targeted therapies (BTT), bilateral tubes, and multiple hospitalizations. Since Emma’s tumor is so rare, she is currently in a trial where she gets 25% less chemo and proton therapy doses. She’s the only one participating in this study because of the rarity of the tumor. Her results will help to change the way cancer is treated.
an MRI was performed two days later. The next day, the tumor was removed during her craniotomy. After a preliminary diagnosis of medulloblastoma that was believed to be cancerous, it was confirmed two days later. Treatment has consisted of a port placement, 30 proton therapy treatments, lumbar puncture, chemotherapy, MRI’s of the spine and head under general anesthesia, bone targeted therapies (BTT), bilateral tubes, and multiple hospitalizations. Since Emma’s tumor is so rare, she is currently in a trial where she gets 25% less chemo and proton therapy doses. She’s the only one participating in this study because of the rarity of the tumor. Her results will help to change the way cancer is treated.
Getting through treatment has been hard on Emma. When she started treatment she was an outgoing sixth grader. Since losing her hair she’s become withdrawn from other children. Despite her difficulties she continues to work diligently on her school assignments and doing Epic Charter School.
 As a result of her diagnosis, Emma suffers from anxiety and depression, decreased fine motor skills and complete left sided deafness. However, Megan says, “She has finally embraced beauty and that it comes in lots of different ways. She is funny and spirited – and yet will lay in my lap and cry often at night.” Emma can be described as ornery, witty and a quick thinker – and her mom wouldn’t have it any other way.
As a result of her diagnosis, Emma suffers from anxiety and depression, decreased fine motor skills and complete left sided deafness. However, Megan says, “She has finally embraced beauty and that it comes in lots of different ways. She is funny and spirited – and yet will lay in my lap and cry often at night.” Emma can be described as ornery, witty and a quick thinker – and her mom wouldn’t have it any other way.
More about Medulloblastoma
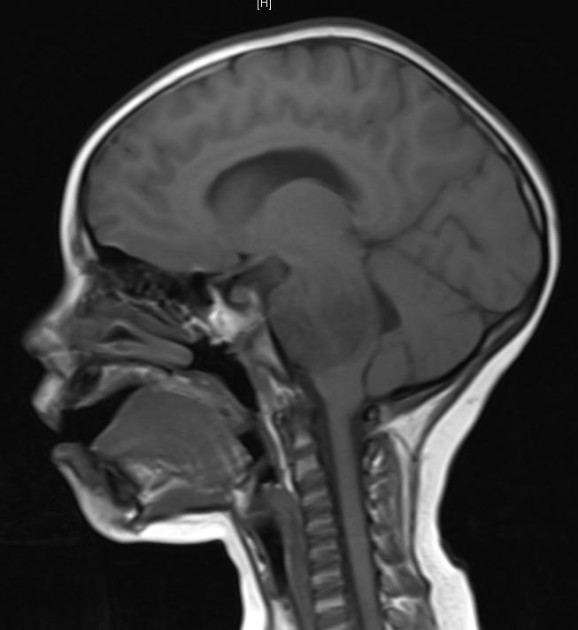
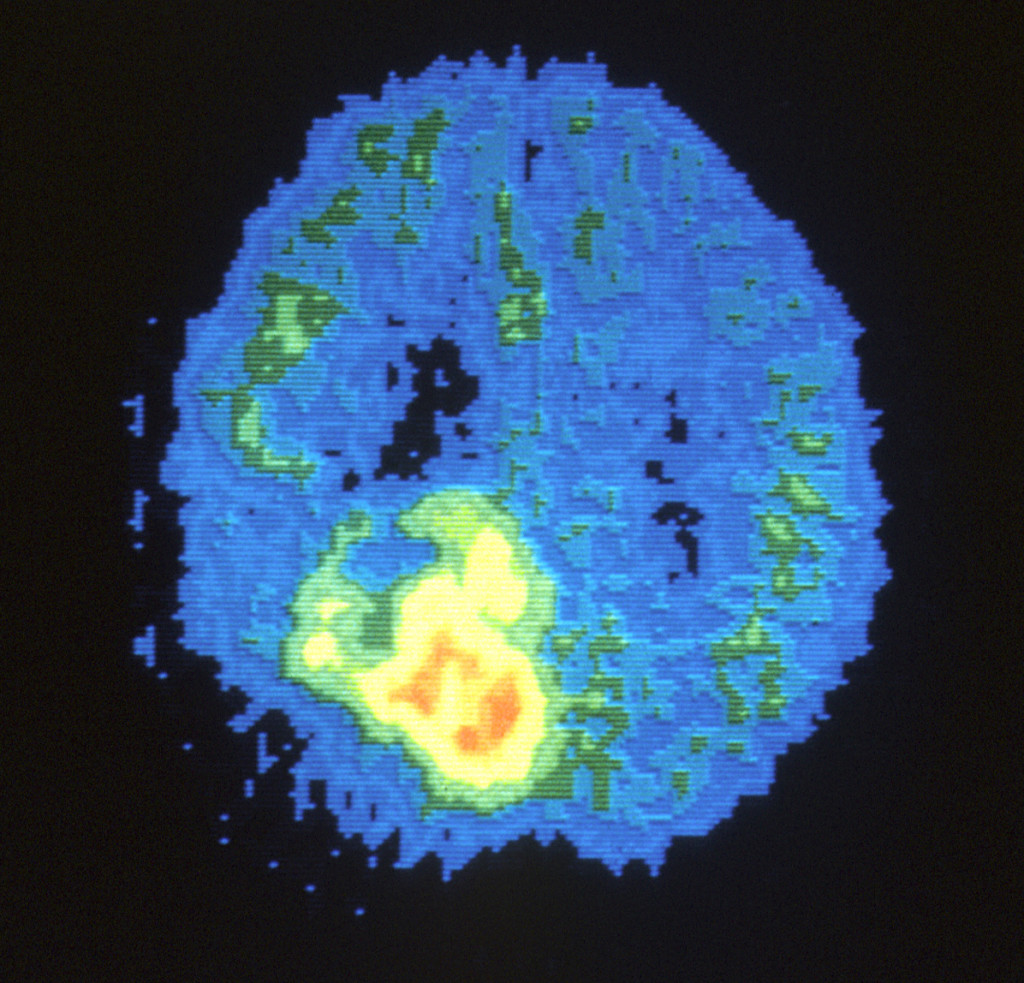
Medulloblastoma is a cancerous (malignant) brain tumor that starts in the lower back part of the brain, called the cerebellum. The cerebellum is involved in muscle coordination, balance and movement.
Medulloblastoma tends to spread through cerebrospinal fluid (CSF) — the fluid that surrounds and protects your brain and spinal cord — to other areas around the brain and spinal cord. This tumor rarely spreads to other areas of the body.
For more information on Medulloblastoma please visit: https://www.acco.org/brain-cancers/
Together, we can make a difference.
Donate today because kids can’t fight cancer alone®.

About American Childhood Cancer Organization
The American Childhood Cancer Organization was founded in 1970 by parents of children and adolescents diagnosed with cancer. As the nation’s oldest and largest grassroots organization dedicated to childhood cancer, ACCO is committed to shaping policy, supporting research, raising awareness, and providing free educational resources to kids with cancer, survivors, and their families. Additionally, ACCO is the sole U.S. member of Childhood Cancer International (CCI) and has helped support more than half a million families over the past 50 years. Help make childhood cancer a national health priority because kids can’t fight cancer alone®.
For more information about how ACCO can help your family, call 855.858.2226 or visit:
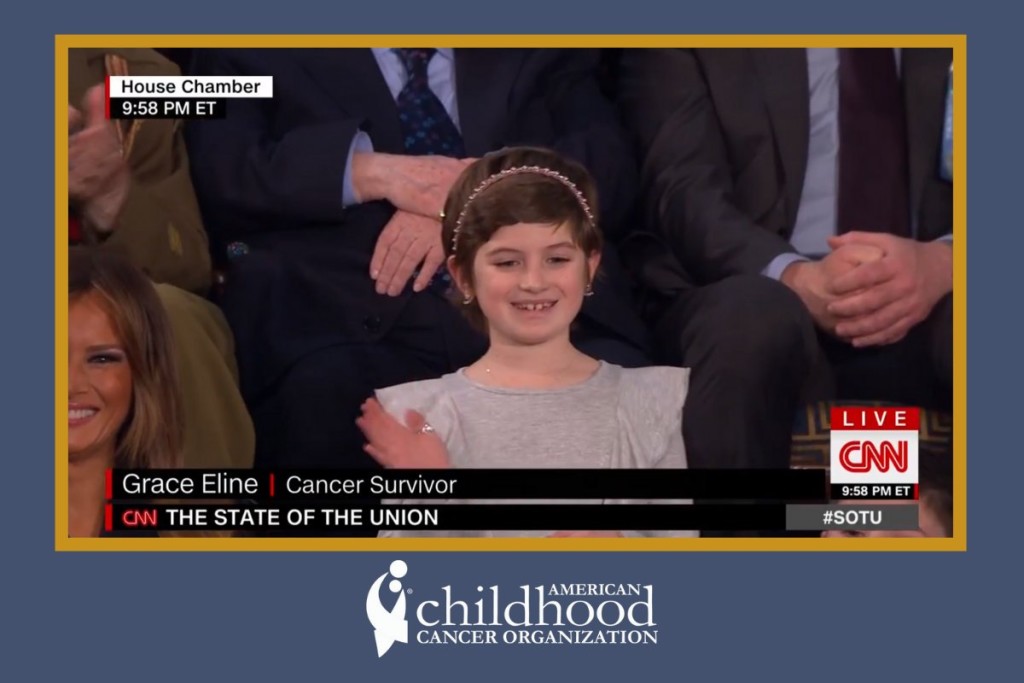 and Amazon + ACCO’s 2018 Ambassador Grace Eline was in the Gallery for the State of the Union speech as an Honored Guest of the President and First Lady.
and Amazon + ACCO’s 2018 Ambassador Grace Eline was in the Gallery for the State of the Union speech as an Honored Guest of the President and First Lady. Beginning in early 2019, our team at ACCO has had several positive and productive meetings with the top leadership at the Department of Health and Human Services (HHS), including HHS Secretary Alex Azar and HHS Assistant Secretary for Health Dr. Brett Giroir. These discussions were unique opportunities to provide decision makers with critical data gathered from our work across the country and around the world. We are grateful to the Administration for giving us a seat at the table and look forward to continuing to share insights and work together.
Beginning in early 2019, our team at ACCO has had several positive and productive meetings with the top leadership at the Department of Health and Human Services (HHS), including HHS Secretary Alex Azar and HHS Assistant Secretary for Health Dr. Brett Giroir. These discussions were unique opportunities to provide decision makers with critical data gathered from our work across the country and around the world. We are grateful to the Administration for giving us a seat at the table and look forward to continuing to share insights and work together.
 ACCO’s team attended Action Days in Washington alongside over 200 other childhood cancer advocates from across the country. In hundreds of meetings on Capitol Hill, Action Day advocates thanked Congress and the Trump Administration for making childhood cancer a national priority and urged them to keep up their important work to ensure full funding for efforts across the board to improve treatments and find cures. Specifically, we called on Members of Congress to fully fund: the National Institutes of Health (NIH) and NCI; the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which was passed into law last Summer; and the President’s Childhood Cancer Initiative.
ACCO’s team attended Action Days in Washington alongside over 200 other childhood cancer advocates from across the country. In hundreds of meetings on Capitol Hill, Action Day advocates thanked Congress and the Trump Administration for making childhood cancer a national priority and urged them to keep up their important work to ensure full funding for efforts across the board to improve treatments and find cures. Specifically, we called on Members of Congress to fully fund: the National Institutes of Health (NIH) and NCI; the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which was passed into law last Summer; and the President’s Childhood Cancer Initiative.
 Is staging relevant for childhood brain tumors? In fact, this is one of the major differences between brain tumors and other types of cancers in children. Regardless of whether they are malignant (cancerous) or benign (non-cancerous), brain tumors in children rarely spread to other organs beyond the central nervous system (which includes the brain and the spinal cord). Therefore, oncologists do not utilize a formal staging system when diagnosing and treating brain cancers.
Is staging relevant for childhood brain tumors? In fact, this is one of the major differences between brain tumors and other types of cancers in children. Regardless of whether they are malignant (cancerous) or benign (non-cancerous), brain tumors in children rarely spread to other organs beyond the central nervous system (which includes the brain and the spinal cord). Therefore, oncologists do not utilize a formal staging system when diagnosing and treating brain cancers. Meet Colton…
Meet Colton…
 According to Shannon, “radiation would only buy us time and there were trials we could participate in, but none were proven to save our child at this point.” During his treatment, Colton had multiple labs done, hospital stays, pneumonia, seizures and eventually lost his ability to walk, talk and swallow. He endured 30 rounds of radiation with a smile on his face. He also participated in a clinical trial for a year at Cincinnati Children’s Hospital.
According to Shannon, “radiation would only buy us time and there were trials we could participate in, but none were proven to save our child at this point.” During his treatment, Colton had multiple labs done, hospital stays, pneumonia, seizures and eventually lost his ability to walk, talk and swallow. He endured 30 rounds of radiation with a smile on his face. He also participated in a clinical trial for a year at Cincinnati Children’s Hospital. 
 The brain is the “command center” for our entire central nervous system, yet despite its critical role in every aspect of human life, it is one of the most delicate organs in the entire body. Any abnormal growth, or tumor, in the brain—whether technically malignant (cancerous) or benign (non-cancerous)—can cause serious damage to the healthy brain tissue and significantly impact the body’s ability to function normally. Therefore, treating a brain tumor requires taking into consideration
The brain is the “command center” for our entire central nervous system, yet despite its critical role in every aspect of human life, it is one of the most delicate organs in the entire body. Any abnormal growth, or tumor, in the brain—whether technically malignant (cancerous) or benign (non-cancerous)—can cause serious damage to the healthy brain tissue and significantly impact the body’s ability to function normally. Therefore, treating a brain tumor requires taking into consideration